![]()
12 THE FOOT AND PASTERN 271
Sue Dyson and Rachel Murray
13 THE FETLOCK REGION 315
Sarah Powell
14 THE METACARPAL/METATARSAL REGION 361
Matthew Brokken, Russell Tucker and Rachel Murray
15 THE CARPAL REGION 385
Sarah Powell and Rachel Murray
16 THE DISTAL TARSAL REGION 405
Sue Dyson
17 THE PROXIMAL TARSAL REGION 421
Rachel Murray, Natasha Werpy, Fabrice Audigié, Jean-Marie Denoix, Matthew Brokken and Thorben Schulze
18 THE STIFLE 451
Carter Judy
19 THE HEAD 467
Russell Tucker, Katherine Garrett, Stephen Reed and Rachel Murray
![]()
Chapter 12
The foot and pastern
Sue Dyson and Rachel Murray
INTRODUCTION
The aims of this chapter are to discuss briefly the indications for magnetic resonance imaging (MRI) of the foot and pastern, to review the current literature, to give an overview of the spectrum of injuries identified at the Animal Health Trust between January 2001 and December 2007 in horses undergoing either low-field or high-field MRI and to provide detailed descriptions of the lesions identified. Where applicable the current knowledge about the nature of these lesions is reviewed.
INDICATIONS FOR MAGNETIC RESONANCE IMAGING
Prior to consideration of MRI, all horses should be subjected to an in-depth lameness evaluation, including local analgesic techniques, high-quality radiography and, where appropriate, ultrasonography and nuclear scintigraphy. Magnetic resonance imaging is an expensive technique and is not required for the diagnosis of all causes of foot and pastern-related pain. However, in the absence of significant imaging findings, MRI is indicated even in the early stages of lameness. Early recognition of the cause of lameness may permit the most appropriate, targeted treatment. A reliable history of a recent, acute puncture wound to the foot is an exception, when MRI may be considered without previous in-depth evaluation.
Local analgesia should be used to define as objectively as possible the source or sources of pain, bearing in mind the current knowledge about the limitations of the majority of local analgesic techniques. Local analgesia is particularly important when acquiring low-field MR images, because the field of view is relatively small and if lameness is not abolished by palmar digital analgesia, then the pastern must be included in the examination. A number of abnormalities may be identified using MRI and interpretation of their relative significance can be facilitated by accurate localization of pain. Likewise the use of nuclear scintigraphy can help to determine the likely clinical significance of lesions identified using MRI, and in some horses may give information about both the nature of the pathological process and the prognosis.
If a flexor cortex defect in the navicular bone is identified radiologically, it is likely that there is associated pathological change in at least the deep digital flexor tendon (DDFT) and such horses may not require MRI to give a prognosis. While MRI could give additional information, the prognosis for such lesions is extremely guarded, and the additional information obtained may have to be balanced against the cost.
SPECTRUM OF INJURY
Five hundred and eighty-four horses were examined at the Animal Health Trust during the study period using low- or high-field MRI, 568 with forelimb lameness and 16 with hind limb lameness. Pain was localized to the digit using local analgesic techniques. In addition to horses with negative imaging findings, horses with the following findings underwent MRI in order to determine better the nature and extent of pathological change:
- ill-defined osseous cyst-like lesions (OCLLs) in the spongiosa of the navicular bone without apparent communication with the flexor (palmar) cortex, or with equivocal radiolucent zones in the flexor cortex of the navicular bone associated with focal, moderate or intense increased radiopharmaceutical uptake (IRU)
- punctate focal core lesions in the DDFT in the pastern, with or without IRU in the region of the DDFT in pool phase scintigraphic images, or at its insertion in the distal phalanx in bone phase images
- enlargement of a collateral ligament (CL) of the distal interphalangeal (DIP) joint with or without change in echogenicity, or with focal IRU in the distal phalanx at the site of insertion of a CL of the DIP joint.
Horses with focal lesions in an oblique sesamoidean ligament (OSL), or a branch of the superficial digital flexor tendon (SDFT), which were considered insufficient to cause the degree of lameness, were also examined. Horses with a previously identified fracture of the distal phalanx or cartilage of the foot were evaluated if concurrent soft tissue pathology, which may influence treatment and prognosis, was suspected. Horses with periarticular new bone around the dorsal aspect of the proximal interphalangeal (PIP) joint which did not respond to intra-articular analgesia were also examined, because other lesions were thought likely be responsible for lameness.
The distribution of injuries is outlined in Table 12.1. This table reflects the cause or causes of lameness considered likely to be of most clinical importance based on the interpretation of the MR images in conjunction with the results of local analgesia (e.g. intra-articular analgesia of the DIP joint, intrathecal analgesia of the navicular bursa) and other imaging modalities (e.g. nuclear scintigraphy). Multiple injuries (i.e. several lesions likely to be contributing to pain and lameness), desmitis of a CL of the DIP joint and DDF tendonitis were the predominant injury categories.
Table 12.1 Distribution of injuries considered to be the primary cause of lameness based on magnetic resonance imaging, clinical findings, response to local analgesia and other imaging modalities in 584 horses with foot pain, January 2001–December 2007
|
| Navicular bone | 21 (3.6) | + 31 horses with multiple injuries, 4 CL DIP joint |
| Navicular bone and DDFT | 60 (10.3) | + 60 horses with multiple injuries, 1 DSL |
| DSIL | 20 (3.4) | + 53 horses with multiple injuries, 5 navicular bone and DDFT, 1 navicular bone, 4 CL DIP joint, 1 distal phalanx |
| CSL | 3 (0.5) | + 57 with multiple injuries, 1 CL DIP joint |
| DDFT | 89 (15.2) | + 52 horses with multiple injuries, 3 primary distal phalanx pathology, 12 CL DIP joint |
| CL DIP joint | 179 (30.1) | + 106 horses with multiple injuries, 15 DDFT, 11 navicular bone and& DDFT, 4 primary distal phalanx pathology |
| SSL | 2 (0.5) | |
| Multiple injuries | 176 (30.1%) | |
| DIP joint | 8 (1.4) | + 10 horses with multiple injuries, 6 CL DIP joint, 1 DSIL |
| Primary injury of the middle and/or distal phalanges | 25 (4.3) | Includes 5 with evidence of previous penetrating injury + 23 horses with multiple injuries, 10 CL DIP joint, 1 navicular bone and DDFT |
All horses with a suspected lesion of the navicular bone, DDFT or a CL of the DIP joint based on conventional imaging techniques were determined to have much more severe lesions on MR images, often with lesions to other structures. A large proportion of lesions of the DDFT that extended proximal to the PIP joint were not detected ultrasonographically. Similarly, ultrasonography failed to detect many lesions of the CLs of the DIP joint, the straight sesamoidean ligament (SSL) and the OSLs.
TYPES OF PATHOLOGICAL CHANGE
Navicular bone
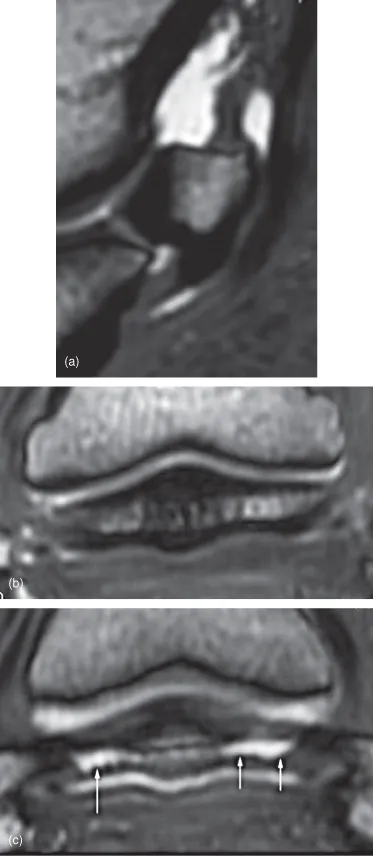
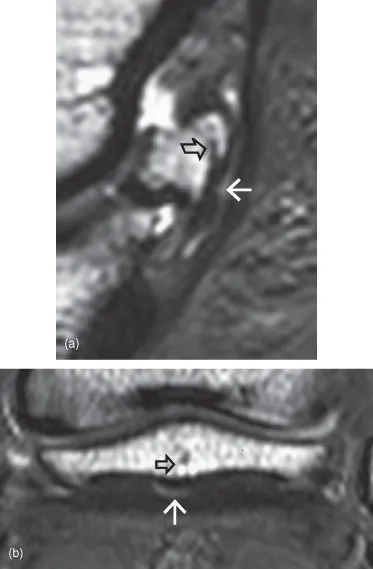
Lesions of the navicular bone are seen alone, in conjunction with injuries of the DDFT, distal sesamoidean impar ligament (DSIL) or collateral sesamoidean ligament (CSL), or as a complex of injuries to multiple structures [1–7]. A comparison of MRI findings in control horses with no history of foot-related pain and horses with chronic palmar foot pain showed significant alterations of the podotrochlear (navicular) apparatus in the lame horses [8]. A comparative MRI and postmortem study showed good correlation between the lesions identified using MRI, gross [9] and histopathological findings [10]. The typical types of lesion identified are summarized in Table 12.2 and illustrated in Figures 12.1–12.8. We believe that there are a number of different pathological processes which can take place within the navicular bone and other components of the podotrochlear apparatus and the DDFT.
Table 12.2 Summary of magnetic resonance imaging abnormalities of the navicular bone
| Distal border | Smooth extension of the distal border into the DSIL
Entheseophyte formation
Irregular thickness of distal cortex with mineralization extending proximally
Enlargement of synovial invaginations
Distal border fragment with no reaction in parent bone
Distal border fragment with change in contour and signal intensity in adjacent navicular bone |
| Proximal border | Entheseophyte formation
Endosteal mineralization
Proximal border fragment |
| Flexor (palmar) border | Endosteal irregularity
Increased thickness of flexor cortex
Focal increased signal in flexor cortex in all image sequences
Focal fluid accumulation palmar to bone consistent with fibrocartilage loss
More extensive loss of fibrocartilage
Linear increase in signal intensity through flexor cortex in STIR images
Focal disruption of flexor cortex, with reaction (abnormal fluid and mineralisation) extending dorsally into the spongiosa
Adhesions of DDFT |
| Dorsal border | Periarticular osteophyte formation
Endosteal mineralization |
| Spongiosa/medulla | Discrete osseous cyst-like lesions in the distal third of the bone
Diffuse increased signal intensity on STIR images
Focal increased signal on STIR images at insertion of CSL and/or origin of DSIL
Linear increased signal on STIR images between insertion of CSL and origin of DSIL
Focal or diffuse decreased signal intensity on T1- and T2-weighted images consistent with mineralization |