- The patient with acute lung injury
- The patient with fever
- The patient with an acute kidney injury
- The patient with long term needs
- The patient with increased intra-abdominal pressure
- The Patient following cardiac surgery
Each chapter develops knowledge of the related physiology/pathophysiology, appropriate nursing interventions that are research/evidence based, technical skills, data interpretation and critical appraisal skills, enabling the reader to apply fundamental knowledge to more complex patient problems. Critical Care Nursing: Learning from Practice is an essential resource for practitioners faced with complex and challenging patient cases.
eBook - ePub
Critical Care Nursing
Learning from Practice
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Critical Care Nursing: Learning from Practice takes a unique approach to critical care. Based around case scenarios that have the patient as the central focus, each chapter is constructed around an example of a critically ill patient with specific care needs. The chapters then go on to critically explore the knowledge and skills required to deliver expert care. This book looks at a range of critical care scenarios, including:
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
The patient with acute lung injury (ALI)
Introduction
Acute respiratory distress syndrome (ARDS) is the severest form of acute lung injury (ALI) and presents one of the greatest challenges to health professionals within critical care. This scenario focuses on the knowledge and skills necessary to manage the complex needs of a patient with ARDS.
Patient scenario
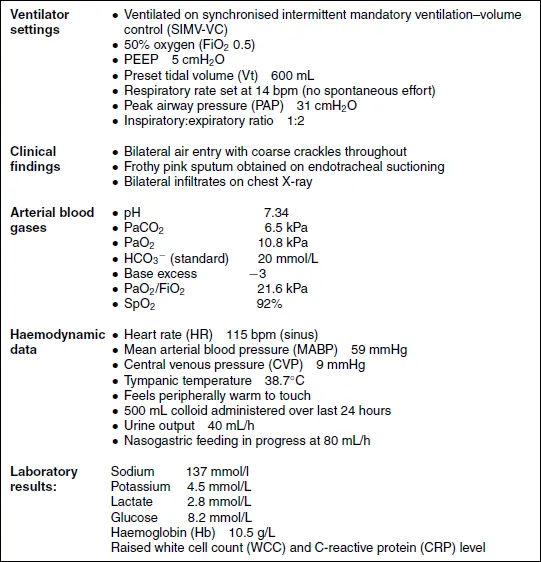
Lee Kuan Yew, a 68-year-old gentleman who weighs 75 kg, was admitted to the intensive care unit (ICU) following intubation in the Accident and Emergency (A&E) department for acute respiratory failure. He had been unwell for four days with shortness of breath, pleuritic pain, fever and rigours and presented to the A&E with tachypnoea, followed by dyspnoea and progressive hypoxaemia and hypercarbia. Physical examination revealed focal findings of consolidation. His past medical history was unremarkable, but he smoked 30 cigarettes per day for the past 40 years. Three days following his admission to the ICU, Lee Kuan Yew remains sedated, intubated and mechanically ventilated. Assessment findings can be seen in Table 1.1.
Reader activities
Having read this scenario, consider the following:
- How do Lee Kuan Yew's symptoms suggest that he has an ALI?
- Consider the possible causes of Mr Kuan Yew's lung injury. Outline the factors that make him at risk for the development of ALI.
- What stage of ALI do you think Mr Kuan Yew is in? Explain this using relevant pathophysiology.
- Analyse the blood gas presented. Consider the possible causes of Mr Kuan Yew's altered results.
- Do you agree with the current ventilation strategy? How would you manage Mr Kuan Yew's respiratory function?
- What therapies other than conventional ventilation can be utilised in the management of ARDS?
Table 1.1 Assessment findings.
Definitions of acute lung injury (ALI) and acute respiratory distress syndrome (ARDS)
Adult respiratory distress syndrome was first described by Ashbaugh et al. in 1967 as a clinical syndrome different from other types of acute respiratory failure, with clinical characteristics of tachypnoea, hypoxaemia resistant to supplemental oxygen, diffuse alveolar infiltrates and decreased pulmonary compliance (Ashbaugh et al. 1967).
Since its initial description in 1967, the criteria for defining ALI/ARDS have changed several times. In 1988 Murray and colleagues proposed a definition which described whether the syndrome was in an acute or chronic phase, the physiological severity of pulmonary injury and the disorder associated with the development of the lung injury (Murray et al. 1988). In 1994, recognising that the study of ALI and ARDS was still hindered by the lack of a simple, uniform definition, the North American–European Consensus Conference (NAECC) published further revised definitions (Bernard et al. 1994) (see Table 1.2).
Table 1.2 American–European Consensus Conference Definitions of ALI/ARDS.
Source: From Bernard et al. (1994).
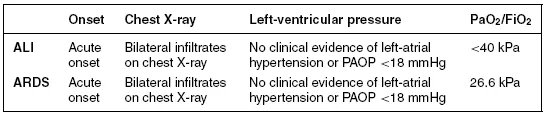
From the NAECC definition it can be deduced that Mr Kuan Yew has ARDS. He has developed acute respiratory failure requiring ventilation; he is hypoxaemic with a PaO2/FiO2 ratio of 21.6 kPa and has bilateral infiltrates on chest x-ray (see Figure 1.1).
Figure 1.1 Chest X-ray. (X-ray courtesy of Dr Duncan Wyncoll, Consultant Intensivist, Guy's and St Thomas’ NHS Foundation Trust, London.)

Mr Kuan Yew does not have a pulmonary artery catheter in situ to enable determination of the pulmonary artery occlusion pressure (PAOP); however, he has no history of cardiac disease and clinically shows no signs of left-atrial hypertension such as a raised central venous pressure (CVP), although the latter can be normal in left-atrial hypertension. Mr Kuan Yew is also demonstrating symptoms of severe sepsis (see Chapter 4 for further information on sepsis), a common co-existing condition.
Pathophysiology of ALI/ARDS
Pathology
In 1972 the National Institute of Health estimated the incidence of ARDS at 60 cases per 100 000 population per year (National Heart and Lung Institute, National Institute of Health (NHL, NIH) 1972). Several robust studies since then have demonstrated a wide range of incidence rates of ARDS from 1.5 to 8.3 cases per 100 000 per year (Villar and Slutsky 1989; Garber et al. 1996). Although it could therefore be considered a rare disease, the mortality of ARDS is high, estimated to be between 34% and 65% (Estenssoro et al. 2002; Herridge et al. 2003). The incidence of ALI, however, appears more common with many patients within high dependency settings having a PaO2/FiO2 of <40 kPa. It is therefore essential that critical care nurses have an understanding of the pathophysiology and management of ALI and ARDS. The major cause of death in patients with ALI/ARDS is multiple organ failure and irreversible respiratory failure, with 84% of deaths occurring more than three days after the onset of ALI/ARDS caused by multi-system organ failure (Ware and Matthay 2000).
Acute lung injury is a term used to describe the response of the lungs to a broad range of insults with ARDS representing the most severe end of the spectrum. Its pathophysiology is driven by an aggressive inflammatory reaction which results in widespread changes throughout the lung. A broad variety of precipitating causes are recognised and these can be differentiated into those which cause injury to the lung directly and those which cause injury indirectly (see Table 1.3). A number of endogenous anti-inflammatory mechanisms are also initiated to counteract the effects of the aggressive pro-inflammatory response; however, these responses may be excessive and contribute to a state of immunoparesis (Doyle et al. 1995).
Table 1.3 Risk factors for ARDS.
| Direct causes | Indirect causes |
|
|
Epidemiological literature indicates that the major risk factor for the development of ALI and ARDS is severe sepsis; 18–40% of patients with sepsis will develop ALI/ARDS, followed by pneumonia, aspiration of gastric contents, multiple blood transfusions, multiple trauma and pregnancy-related ALI/ARDS (Villar and Slutsky 1989; Ware and Matthay 2000).
From Mr Kuan Yew's clinical history and initial presentation it appears that he may have developed an acute lung injury and subsequent ARDS from a direct cause such as lobar pneumonia. It is also important, however, to note that as Mr Kuan Yew is mechanically ventilated and is critically ill, he is at a significant risk of developing a nosocomial infection and secondary sepsis (Vincent et al. 1995), a major risk factor for the development of ARDS, and at present he is indeed demonstrating signs of severe sepsis.
ALI and ARDS cause diffuse alveolar damage affecting all parts of the alveolus, including the epithelium, the endothelium and the interstitial space. It is a progressive condition with the pathological changes typically described as passing through three overlapping phases – an inflammatory or exudative phase, a proliferative phase and a fibrotic phase (Ware and Matthay 2000).
Exudative phase
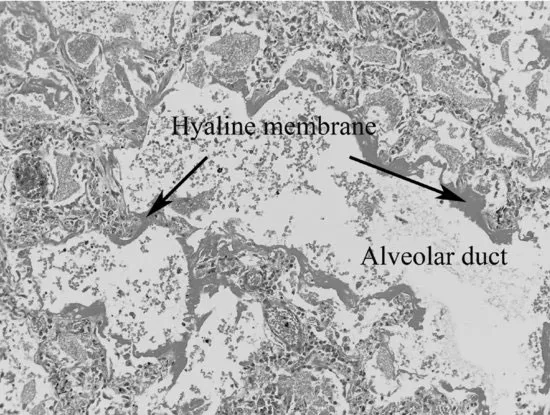
Lasting for up to seven days following the onset of symptoms, the exudative or acute phase of ALI/ARDS is characterised by the influx of protein-rich oedema fluid into the alveolar air spaces, as a result of increased permeability of the alveolar–capillary membrane and the formation of hyaline membranes. The hyaline membranes contain necrotic epithelial cells, plasma proteins which have been deposited in the alveolar space as part of the inflammatory exudate that leaks across the alveolar–capillary membrane, immunoglobulin and complement. The alveolar–capillary barrier has focal areas of damage and the alveolar wall is oedematous. Neutrophils are increasingly found within the capillaries, interstitium and eventually airspaces. As the process of damage progresses, there is extensive necrosis of type 1 alveolar epithelial cells and further hyaline membrane formation (Figures 1.2a and 1.2b).
Figure 1.2 (a) Histopathology slide of lung tissue. (b) Diagrammatic illustration of cellular changes in ARDS. (Baudouin 2004). Used with permission of Massachusetts Medical Society.
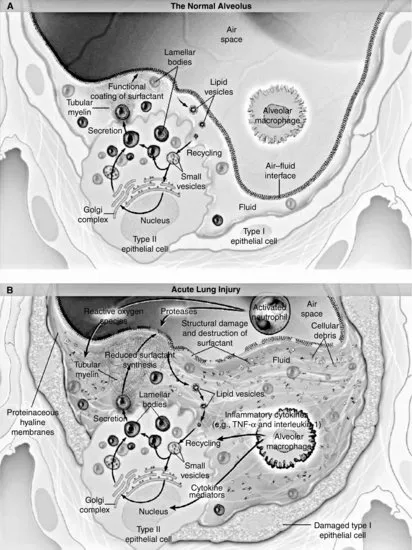
These pathological changes can be seen in Mr Kuan Yew's clinical picture by the presence of pulmonary oedema and his deterioration in lung function. Flooding of the alveoli with protein-rich fluid and debris has caused a decrease in lung compliance, reflected in the high airway pressures. It has also caused a significant reduction in the diffusion of oxygen, leading to a reduced arterial oxygen saturation and PaO2. Fluid-filled and collapsed alveoli result in the development of a right to left intra-pulmonary shunt. The negative effects of this on Mr Kuan Yew's gas exchange are further compounded by loss of the normal compensatory hypoxic pulmonary constriction.
Proliferative phase
The proliferative phase is characterised by organisation of the hyaline membranes by proliferating fibroblasts, cell debris and inflammatory cells (Ware and Matthay 2000). Necrosis of type 1 alveolar cells exposes areas of the epithelial basement membrane and the lumens of the alveoli fill with leucocytes, red blood cells and fibrin. Type 2 alveolar cells, which are responsible for the production of surfactant, are also damaged but some proliferate along the alveolar wall in an attempt to cover damaged areas of the epithelium and differentiate into type 1 cells. Pulmonary oedema is less prominent at this stage; however, alveolar collapse becomes more marked and the alveolar ducts become narrowed and distorted. This then leads to a further increase in the degree of intrapulmonary shunt, leading to a further deterioration in gas exchange, and hypoxaemia resistant to oxygen therapy.
At this stage the process can be reversed and the lung parenchyma may return to normal. However, in some cases the damage is severe and the hyaline membranes become incorporated into the walls of the revised alveoli (Ware and Matthay 2000).
Fibrotic phase
The fibrotic phase can begin as early as ten days following the insult and is characterised by progressive thickening of the vasculature walls and an increase in the amount of lung collagen (Ware and Matthay 2000). Fibrosis results in a further reduction in lung compliance, increasing the work of breathing, decreasing the tidal volume and resulting in the retention of CO2. As a result of the destruction of some alveoli and interstitial thickening, gas exchange is reduced and this contributes to further hypoxaemia and ventilator dependence.
Pathogenesis of ALI/ARDS
Inflammation
As a result of the initiation of an inflammatory response, there is increased leucocyte production and mobilisation to the inflamed site. Mediator cascades including the production of cytokines, chemokines, free radicals and complement and coagulation pathway components are also activated. There is also an anti-inflammatory response.
The neutrophil is the dominant leucocyte involved in the pro-inflammatory response. Neutrophils cause cell damage by the production of free radicals, pro-inflammatory mediators and proteases, and excessive quantities of these products, including cytokines, have been found in patients with ARDS (Chollet et al. 1996). The inflammatory response is in part driven by cytokines. Two of the major pro-inflammatory cytokines are tumour necrosis factor-α (TNF-α) and interleukin-1 (IL-1). The actions of these include (1) recruitment and localisatio...
Table of contents
- Cover
- Title Page
- Copyright
- Contributor list
- Preface
- Acknowledgements
- Chapter 1: The patient with acute lung injury (ALI)
- Chapter 2: The patient requiring complex weaning from mechanical ventilation
- Chapter 3: The patient with fever
- Chapter 4: The patient with severe sepsis
- Chapter 5: The patient following cardiac surgery
- Chapter 6: The patient with severe upper gastrointestinal bleeding due to oesophageal varices
- Chapter 7: The patient with altered blood glucose
- Chapter 8: The patient with increased abdominal pressure
- Chapter 9: The patient with an acute kidney injury
- Chapter 10: The patient in acute pain
- Chapter 11: The patient requiring sedation
- Chapter 12: The patient with raised intracranial pressure
- Chapter 13: The patient with delirium
- Chapter 14: The patient with seizure activity
- Chapter 15: The patient following poisoning
- Chapter 16: The patient with long-term needs
- Chapter 17: The patient requiring end-of-life care
- Appendices
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Critical Care Nursing by Suzanne Bench, Kate Brown, Suzanne Bench,Kate Brown in PDF and/or ePUB format, as well as other popular books in Medicine & Nursing. We have over 1.5 million books available in our catalogue for you to explore.