![]()
Chapter 1
Introduction
Peter Thomson
General Introduction
This book deals with the diagnosis and management of oral precancer, a relatively rare but important and fascinating range of potentially malignant disorders. Oral precancer comprises both discrete, readily identifiable, oral mucosal lesions such as leukoplakia or erythroplakia and also more widespread or systemic conditions that may affect the lining of the oral cavity, and whose clinical presence may precede the development of invasive oral cancer.
The concept of a recognisable precancer state has arisen following a number of salient clinicopathological observations that include the observed transformation of pre-existing clinical lesions into invasive cancers during patient follow up, the recognition that leukoplakic or erythroplakic lesions are often found to coexist with oral squamous cell carcinoma, and the realisation that numerous histopathological and biomolecular tissue changes are actually common to both cancers and their potentially malignant counterparts [1].
The identification of a potentially malignant disorder in an individual patient, however, does not mean that an inevitable malignant transformation will take place because many of these oral lesions do not progress over time and some may even resolve or regress spontaneously. Nonetheless, statistically, such patients are known to remain at an increased risk of developing mouth cancer.
Cancer of the mouth, which is primarily a squamous cell carcinoma arising from the oral mucosa lining, is the sixth most common cancer worldwide and is traditionally seen most frequently in older people [2]. It is a lethal and deforming disease due not only to local tumour invasion, oro-facial tissue destruction and cervical lymph node metastasis, but also because of widespread blood-borne tumour dissemination affecting particularly the lungs and the liver. Worldwide, 5-year survival rates for oral cancers are around 50%, with prognosis worsening with advanced disease and late presentation [2].
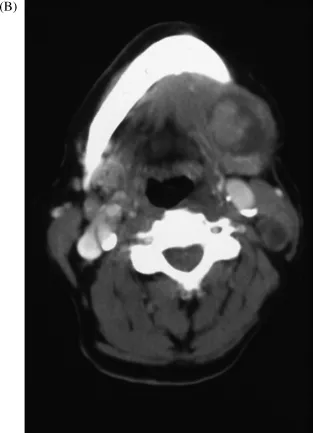
Figure 1.1 shows a typical clinical presentation of a large, invasive, squamous cell carcinoma arising posteriorly in the retromolar and palatoglossal regions of the oral cavity (Figure 1.1A), together with an accompanying computed tomography (CT) scan demonstrating extensive tumour spread to the draining cervical lymph nodes (Figure 1.1B). As is often the case, the patient presented late on in the progress of the cancer disease, having been relatively asymptomatic for many months. Of interest in this case are the surrounding mucosal precancer changes of leukoplakia (clearly visible in Figure 1.1A) that may well have preceded the malignancy.
So, despite real advances in diagnosis and management, nearly half of all patients diagnosed with an oral malignancy will die as a direct consequence of their disease. Whilst the number of patients suffering uncontrolled cancer disease at primary sites in the head and neck has reduced in recent years due to improvements in modern treatment protocols, up to a quarter of patients may then go on to develop multiple cancers in the upper aerodigestive tract either synchronously (at the same time) or metachronously (separated by time).
The presentation of multiple lesions in an individual patient is an illustration of widespread epithelial cell instability, which is a hallmark of head and neck squamous carcinoma, and is classically referred to as ‘field change’ cancerisation. This was the term first proposed by Slaughter in 1953, who proposed that oral cancers developed in multifocal areas of precancer change as a result of widespread abnormalities in the aerodigestive tract epithelium [3]. More recent observations suggest that the risk of multiple primary cancer development is probably highest in younger patients and particularly in those who continue to smoke and consume alcohol following treatment interventions [2].
Aetiological factors causing malignant transformation of oral stratified squamous epithelium most commonly involve the excessive consumption of tobacco products and alcohol misuse, ultimately presenting clinically as symptomatic tumours in a predominantly elderly male population. In recent years, however, there has been a definite rise in the incidence of oral cancer with higher rates appearing in younger and in female patients. Indeed, no other cancer site has shown such a rapid rise in incidence over the last 25 years and some researchers predict an epidemic of oral cancer occurring during the first half of the 21st century.
Of course, many people who smoke and drink do not develop oral cancer and similarly in a number of other studies it has also been observed that many oral cancer patients may not have been overexposed to tobacco or alcohol at all, so it remains imperative to identify and determine the significance of other potential risk factors. Genetic predisposition to DNA mutation in oral epithelial cells, poor nutrition characterised by a low intake of fresh fruit and vegetables, ageing, low socioeconomic status, poor oral health and infection have all now been implicated in oral carcinogenesis [4].
More recently, a significant role for human papillomavirus (HPV) infection (especially subtype 16) has been postulated in oral carcinogenesis, although this seems to be particularly associated with a rise in oropharyngeal, tonsil and tongue base cancer. This seems to affect young patients in particular, often presenting with extensive cervical lymph node metastases and may be associated with a sexually transmitted aetiology. HPV-associated head and neck cancer may thus represent a distinct disease entity of its own [5, 6].
Although HPV DNA has been identified in samples of leukoplakia, the precise role of HPV in the initiation and progression of oral potentially malignant disease remains somewhat obscure and is currently the subject of a number of ongoing investigations.
The ‘progression model’ for oral carcinogenesis suggests that, following genetic mutation, various phenotypic epithelial tissue disorganisation and dysmaturation changes occur, which if allowed to progress ultimately lead to carcinoma development and invasive disease. Such disorganised features preceding cancer are identifiable at the microscopic level and are described collectively as epithelial dysplasia.
Dysplasia is thus a crucially important histopathological entity that delineates the many structural changes that affect both individual epithelial cells and also the overall integrity of epithelial tissue hierarchy present in potentially malignant lesions. An estimate of the degree of dysplastic change present in the epithelium is made following lesion biopsy and is classified into mild, moderate or severe categories. The more severe the dysplasia, the higher the risk there is for malignant change, although there is a strong subjective element in dysplasia grading and both biopsy sampling errors and possible fluctuations in severity with time may all confound the accuracy of diagnosis.
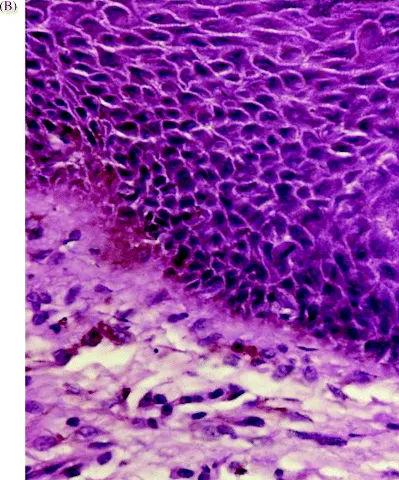
It has been recognised for many years that a spectrum of distinct oral mucosal abnormalities which may accompany these dysplastic changes can be identified clinically and characterised, albeit somewhat non-specifically, during an oral examination. Figure 1.2 illustrates both the clinical appearance of a diffuse, non-homogenous leukoplakic lesion arising on the ventrolateral tongue mucosa (Figure 1.2A), and its corresponding dysplastic appearance under the microscope (Figure 1.2B).
Fortunately, with the application of a good light source, the oral cavity is easily visualised directly during clinical examination and, indeed, is inspected regularly by dental practitioners during routine dental care. There is, thus, potential for both early diagnosis and therapeutic intervention during this clinically identifiable ‘oral precancer window’.
In order to improve survival rates for oral cancer we must therefore avail ourselves of this ‘window’ to identify precancer change at the earliest possible stage and attempt to intervene to halt the disease process. Unfortunately, there is considerable public ignorance regarding oral cancer, the patient population that is probably most at risk rarely attends for regular oral examination, and general population screening programmes for oral cancer have been found to be fundamentally flawed as a health care intervention.
On the other hand, the identification and targeting of individuals at high risk of developing cancer may provide a more practical solution. For example, it has been shown that many irregular patient attendees who only ever visit dental access centres for emergency treatments are often those with the lifestyle habits that render them most vulnerable to oral cancer. Thus focused oral cancer screening and health care information may be most effectively targeted to this type of at-risk population group [7].
The currently available scientific literature is also unable to resolve the fundamental question as to whether early diagnosis and treatment of precancerous conditions will ultimately prevent the development of malignant disease. It is not, however, an unreasonable hypothesis and provides a proactive interventional technique that will be discussed in some detail later in this book.
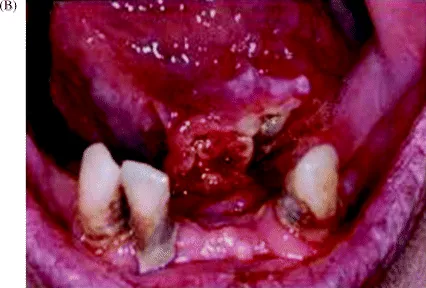
A further problem to consider is that, having identified potentially malignant disorders, we are unable to predict the clinical behaviour of any individual patient or precancer lesion. This common clinical dilemma and its unfortunate consequences are illustrated in Figure 1.3.
There are also no clear management guidelines or agreed treatment strategies for oral precancer cases. The lack of meaningful, randomised controlled clinical trials has resulted in a variety of proposed treatments that are essentially based on clinicians' preferences and experience.
In order to try to address some of these longstanding dilemmas, this book will attempt to concisely review current concepts of oral precancer disease, epithelial cell biology and oral carcinogenesis and its related pathology to try to improve our understanding of this complex and fascinating oral oncology pathway. Utilising a number of longitudinal patient cohort studies, we will also outline our preferred diagnosis and management strategy for potentially malignant disorders and explain our rationale for clinical decision making and treatment selection. It is hoped that in this way we can make a significant contribution to the ongoing scientific debate surrounding oral precancer disease and also help to improve the clinical care and outlook for our many patients that present with these important, potentially malignant and life-threatening oral conditions.
Epidemiology
Studies on the causation, distribution and control of disease form the backbone of epidemiological research. The majority of...