![]()
1
What Every Emergency Physician Must Know
People from many different backgrounds, with an enormous variety of problems, present to an emergency department (ED) both by day and by night. Fortunately, certain basic principles are applicable to the care of them all.
WHAT TO DO IN AN EMERGENCY
In all cases, swift and accurate assessment must immediately lead to appropriate action:
Cardiac arrest → p. 150.
Children → p. 329.
A – Airway
The airway may be:
- patent, partially obstructed or completely obstructed (this results from physical obstruction or loss of muscle tone)
- adequately protected or at risk (this depends on the protective reflexes of the airway).
Check for Responsiveness
Is the patient alert and responsive to questions? A verbal reply confirms that there is:
- a maintained and protected airway
- temporarily adequate breathing and circulation
- cerebral functioning.
If responsive, then the patient will usually be able to elaborate on the cause of the sudden deterioration that has brought him or her to an ED.
Failure to respond indicates a significantly lowered level of consciousness and therefore an airway that may be obstructed and is definitely at risk. There may be a need for airway-opening manoeuvres and action to protect the airway.
Look, Listen and Feel for Breathing
The absence of breath sounds indicates the need to attempt airway-opening manoeuvres (see below) and if unsuccessful to consider the possibility of a foreign body obstruction.
Foreign body obstruction may initially present as a distressed, very agitated, cyanosed patient – ‘choking’.
Cardiorespiratory arrest → p. 150.
Choking → p. 196.
Respiratory arrest → p. 199.
If breathing is present then do the following.
Look for the Signs of Partial Upper Airway Obstruction
- Snoring: the familiar sound of obstruction caused by the soft tissues of the mouth and pharynx. Often it accompanies the reduced muscle tone of a lowered level of consciousness.
- Rattling or gurgling: the sound of fluids in the upper airway.
- Stridor: a harsh, ‘crowing’ noise, which is heard best in inspiration. It is thus different from wheezing, which is usually loudest in expiration. Stridor suggests obstruction at the level of the larynx and upper trachea. General illness and temperature usually indicate an infection causing swelling. Obstruction by a foreign body is the other main cause.
In cases of suspected supraglottic swelling, examination or instrumentation of the throat should not be carried out for fear of causing complete obstruction.
- Drooling: the inability to swallow saliva. It suggests blockage at the back of the throat.
- Hoarseness: gross voice change. This suggests obstruction at the level of the larynx.
Cyanosis and reduced haemoglobin saturation readings on a pulse oximeter are very late signs of airway obstruction.
Allergic reactions → p. 299.
Laryngotracheal obstruction → p. 196.
Surgical airways → p. 22.
Assess the need for cervical spine protection before any airway intervention.
Clearance and Maintenance of the Airway
A patent airway is a prerequisite for life; a blocked airway is a common harbinger of death in emergency situations. There are two main ways in which the airway becomes blocked.
1 Depressed level of consciousness: most common cause. The tone of the muscles controlling the patency of the mouth and the pharynx is under neural control, in much the same way as the activity of the other striated muscles of the body. When this control is lost, the soft tissues around the airway prolapse and fail to maintain patency (simplistically, the tongue falls back).
This is overcome by:
- tightening these tissues (chin-lift manoeuvre)
- pushing the jaw and the hyoid bone and their attached soft tissues forward (jaw-thrust manoeuvre)
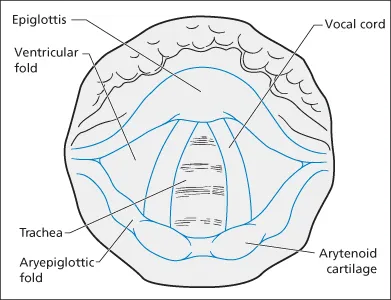
- putting an artificial airway down the anatomical airway (oro- or nasopharyngeal airways, endotracheal tubes, laryngeal masks, etc. → Figure 1.1).
2 Physical obstruction: many things can do this (direct trauma, external or intramural mass, etc.) However, in emergency practice, there is usually either something in the airway (vomitus, blood or foreign body) or there is swelling in the wall of the airway (oedema, haematoma, etc.).
This is overcome by:
- removing the cause of the obstruction (suction, manual removal or choking manoeuvres)
- passing an artificial airway (as detailed above) past the obstruction
- reducing the swelling with vasoconstrictor drugs (adrenaline)
- bypassing the obstruction with a surgical airway.
Protection of the Airway
The airway is normally kept clear of foreign matter by the gag, cough and laryngeal reflexes. These may be attenuated by specific palsies, the effects of drugs or a generalised depression of conscious level. They may also be impaired at the extremes of age and in states of general debilitation. Special vigilance is required in all such situations; the recovery position should be used whenever possible.
Paradoxically, these same reflexes may make advanced airway care extremely difficult in situations where they are not completely absent. At such times, the airway should be managed by a person skilled in both its assessment and the use of sedating and paralysing drugs.
Over 10% of normal individuals have no gag reflex.
Laryngospasm, bleeding, vomiting and consequent hypoxia can result from ill-judged attempts at intubation. It should be noted that the absence of the gag reflex is not a good predictor of the need for (or the ease of) endotracheal intubation.
In a patient with a reduced level of consciousness, the airway must be assumed to be at risk until proved otherwise.
On-going protection of the airway requires continual vigilance. The following are also essential:
- The recovery position uses gravity, both to drain fluid matter away from the airway and to allow the soft tissues to be positioned in such a way that they do not cause obstruction. Once the airway is clear, this position can be used to both maintain and protect the airway.
- A high-flow suction catheter must always be near the patient’s head.
- The patient’s trolley must be capable of tilting ‘head down’ so as to drain vomitus out of the airway.
- If endotracheal intubation is attempted, the airway must be protected by the manoeuvre known as cricoid pressure throughout the period of instrumentation. Pressure is applied to the front of the patient’s cricoid cartilage by an assistant using the thumb and two fingers. This compresses the oesophagus against the cervical spine and thus prevents the passive regurgitation of gastric contents. The airway is vulnerable from the start of induced paralysis until the cuff is i...