![]()
SECTION 1
Assessment and Treatment
![]()
CHAPTER 1
Assessment
Jose M. Menchon
Department of Psychiatry, Hospital Universitari de Bellvitge-IDIBELL, Hospitalet de Llobregat (Barcelona), Universitat de Barcelona, CIBERSAM, Spain
INTRODUCTION
Many people have some obsessions during their lives: it is estimated that more than one-quarter of people experience obsessions or compulsions at some time [1], and a substantial proportion of them will meet the criteria for obsessive-compulsive disorder (OCD). The lifetime prevalence of OCD is about 2–2.5%, and the annual prevalence is 1–2% among the general population [1,2]. The male to female ratio is approximately unity, with some studies finding a slightly higher prevalence in women, while in the child and adolescent populations males show a higher prevalence.
The hallmark of OCD is the presence of either obsessions or compulsions. According to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) [3] diagnostic criteria, the obsessions are defined by the following four criteria:
1. Recurrent and persistent thoughts, impulses or images that are experienced, at some time during the disturbance, as intrusive and inappropriate and that cause marked anxiety or distress.
2. The thoughts, impulses or images are not simply excessive worries about real-life problems.
3. The person attempts to ignore or suppress such thoughts, impulses or images, or to neutralize them with some other thought or action.
4. The person recognizes that the obsessional thoughts, impulses or images are a product of his or her own mind (not imposed from without as in thought insertion).
Compulsions are defined as: ‘1) repetitive behaviors (e.g., hand washing, ordering, checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to rules that must be applied rigidly, and 2) the behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation; however, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive.’ Hence, obsessions and compulsions are repetitive, unpleasant and intrusive (although recognized as own thoughts), and usually the individual considers that the obsessions or compulsions are excessive or irrational, demonstrated by the subject’s attempts to resist them. While obsessions are considered phenomena that increase anxiety or discomfort, compulsions are behaviours that are aimed at reducing it.
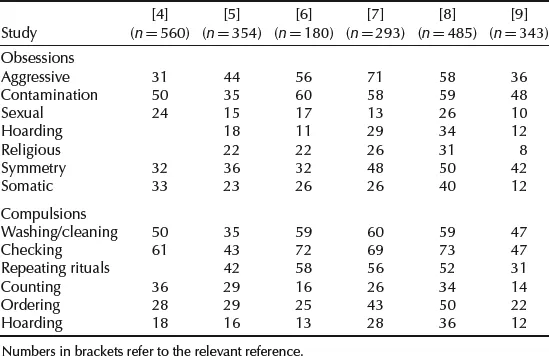
Obsessions and compulsions are very diverse and have been grouped into various types. Table 1.1 shows the percentage of obsessions and compulsions in adult OCD samples reported in several studies. Such diversity in the clinical manifestations of OCD has led researchers to examine whether the different obsessions and compulsions seen in patients could be related and grouped into a few subtypes or dimensions; for instance, a recent meta-analysis [10] has derived four main factors: symmetry, forbidden thoughts, cleaning and hoarding. Apart from its descriptive utility, this kind of approach has heuristic value since it allows examination of the possible heterogeneity of OCD in terms of neurobiology, genetics or treatment response, among other aspects [11]. This issue is reviewed in detail in Chapter 6 of this book.
Table 1.1 Percentage of obsessions and compulsions in OCD adult samples reported in various studies.
The assessment of OCD includes the usual elements involved in the psychiatric assessment of mental disorders, although there are also specific issues related to this condition. Relevant issues in the OCD assessment are (Table 1.2):
Table 1.2 Components in the assessment of OCD.
Clinical Assessment Present obsessive-compulsive symptoms: subtype/dimensions of symptoms; severity; degree of insight Risk of suicide Cognitive biases and behavioural analysis (how does the patient behave in response to obsessions? What kind of obsessions elicits compulsions? How much associated anxiety is there? Is there any resistance to and control over compulsions?) Neuropsychological dysfunctions Conditions associated with the onset and course of the symptoms: past or present history of tics or Tourette disorder; possible history of PANDAS (Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal infections); relationship of the disorder with reproductive events (onset or worsening of symptoms at the menarche, pregnancy and other reproductive events); relationship with life events Course of the disorder: age at onset of the first symptoms and of the disorder, degree of stability of the subtype of symptoms (have always been the same type of symptoms?), age at first treatment, type of evolution (episodic, chronic or fluctuating, progressive improvement or worsening), degree of functional impairment Personality traits or disorders Differential diagnosis of other disorders and comorbidities: organic brain disorders, schizophrenia, depression, hypochondriasis, phobias, Tourette or tic disorder, obsessive-compulsive personality disorder, body dysmorphic disorders, grooming disorders (trichotillomania, skin picking disorder), hoarding, presence of other obsessive-compulsive spectrum disorders Family assessment: family history of psychiatric disorders, degree of support from relatives, degree of understanding of the disorder by relatives, ability of the relatives to participate in the treatment Treatment: previous drug treatments (doses and duration), previous psychological therapies, response to previous treatments (remission, partial response, no response) |
- the instruments for detecting and diagnosing the disorder;
- the examination of the obsessive-compulsive (OC) symptoms: the severity and type of symptoms, the level of insight, cognitive biases and behavioural analysis;
- the assessment of the suicide risk;
- the appraisal of neuropsychological functions;
- differential diagnosis;
- the presence of comorbid and related/spectrum disorders;
- the review of the course of the disorder: age of onset of OC symptoms, age at which the subject met diagnostic criteria for OCD, type of course of the disorder (e.g. episodic, chronic with or without fluctuations, progressive worsening);
- the analysis of the response to previous treatments, including both clinical outcome and degree of disability of the patient’s functioning.
Given that some of the components of the assessment are examined in other chapters, the present review will focus on the detection of OCD, the clinical rating of OC symptoms, the assessment of insight and the suicide risk, the differential diagnosis, and OC related and spectrum disorders.
DETECTING OCD
Many OCD sufferers experience shame about their symptoms or think that these will be misunderstood as ‘madness’, while others may even be afraid that their symptoms do actually mean that they are becoming ‘mad’. For some patients these symptoms may be stigmatizing while others do not view their symptoms as a disorder, lacking insight of their morbid nature; others may think that they do not require treatment. All these beliefs and attitudes reduce the likelihood of disclosing their OCD symptoms to their physicians. A study of attitudes towards OCD symptoms [12] showed that the attitudes may vary across the different symptoms of the disorder, finding that obsessions related to harm were the most feared and unacceptable, followed by the washing behaviour, and then the checking behaviour. Therefore, fear of the meaning of the obsessions/compulsions, embarrassment about reporting them, viewing them as stigmatizing, or lacking insight into their nature, may all delay seeking help for them. This delay was evident in the study by Pinto et al. [7], which found that the time elapsed between the first symptoms and the first treatment was 17 years, and that between meeting the diagnostic criteria for OCD and the first treatment was 11 years.
The importance of adequate recognition of OCD is reflected in a study in which only 30.9% of severe OCD cases received a specific OCD treatment [1], although 93% of the patients reported that they were receiving mental health treatment in some kind of health setting (general medical, mental health settings, human services or complementary/alternative medicine). The data were more striking in patients with moderate OCD, since only 2.9% of this group of patients were on specific OCD treatment while 25.6% of this group were receiving mental health treatment.
These data regarding attitudes to OCD symptoms, and therefore the delay in both receiving an OCD diagnosis and starting an adequate treatment, emphasize the importance of the strategies to detect OCD.
Screening in clinical interview
Some patients with OCD will describe their symptoms quite well, and diagnosing OCD will not be difficult provided that the phys...