![]()
Chapter 1
Definition of orthodontics and factors influencing orthodontic treatment
Orthodontics is a specialised branch of dentistry. The name comes from two Greek words:
- orthos – meaning straight or proper
- odons – meaning teeth
so the meaning is clear – ‘straight teeth’.
Orthodontics is the study of the variations of the development and growth of the structures of the face, jaws and teeth, and of how they affect the occlusion (bite) of the teeth.
Ideally, there should be the same number of permanent teeth in each arch.
Any deviation from the norm is called:
- a malocclusion, if it affects teeth alignment and the bite relationship
Most malocclusions are genetically caused, i.e. they are inherited, e.g. missing teeth or a protruding mandible.
Other malocclusions can be caused by the patient, e.g. digit sucking or trauma.
Orthodontic treatment can correct a malocclusion by putting the teeth into their normal position and occlusal relationship (with surgical help, if needed) so that:
- the bite is fully functioning and the patient can bite and chew properly
- the oral hygiene is made easier, thus helping to prevent caries and gingivitis
- the malocclusion does not cause other damage
- the patient looks better and has better self-esteem
Orthodontic treatment in conjunction with orthognathic (maxillo-facial) surgery can correct an underlying jaw discrepancy or facial asymmetry.
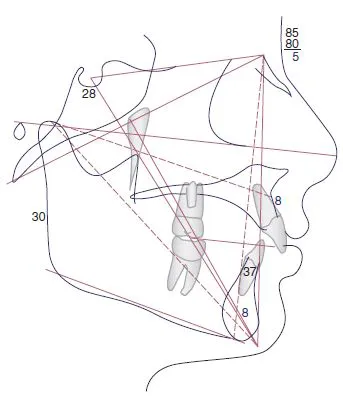
Orthodontic planning is done in conjunction with the surgeons using clinical and radiographic assessment, with a cephalometric tracing (Figure 1.1) often analysed using computer software program.
So, orthodontists set out to:
- straighten teeth
- improve the bite
- improve the function
- improve oral hygiene (and make teeth easier to clean)
- improve self-esteem of the patient
CLASSIFICATION OF OCCLUSION
When assessing occlusion there are two aspects to classification:
- incisor relationship
- buccal segment occlusion, left and right
Both are recorded on a patient’s Orthodontic Assessment Form.
Incisor classification
- Classes have roman numerals, e.g. I, II, III
- Divisions do not, e.g. Class II/1 or Class II/2
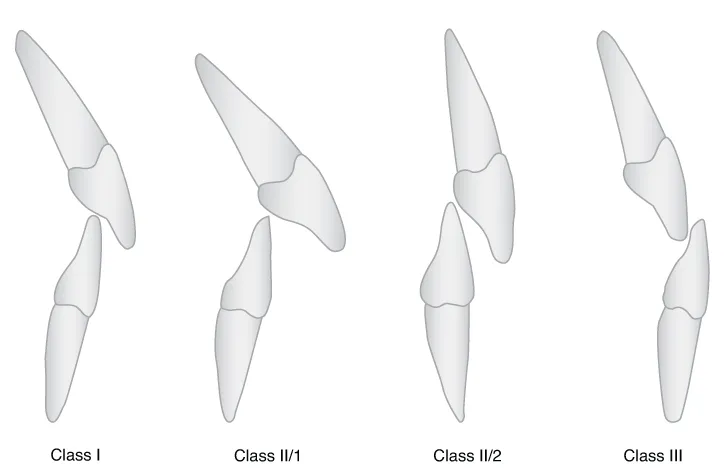
The incisor classification (Figure 1.2):
- relates to the bite of the tip of the lower central incisors onto the back of the upper central incisors
- is divided into three horizontal sections and where the lower incisor occludes will determine the classification
Class I
- The incisal edge of the lower incisors bites on or below the cingulum plateau of the upper incisors
Class II/1
- The upper incisors are proclined or upright (Figures 1.3 and 1.4)
- The lower incisors bite behind the cingulum plateau of the upper incisors
- The position of these front teeth means they can be damaged more easily because of their vulnerable position
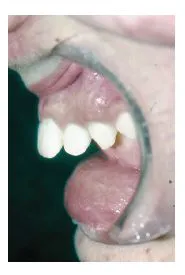
Class II/2
- The upper incisors are retroclined
- The lower incisors bite behind the cingulum plateau
- The position of the teeth can, when closed, lead to trauma to the lower labial gingivae and the upper palatal gingivae (Figures 1.5-1.7)
Class III
- The bite is edge to edge or reversed
- The incisal edge of the upper incisors can bite into the back (lingual) surface of the lower incisor (Figure 1.8)
- A horizontal overlap is called overjet
- A vertical overlap is called overbite
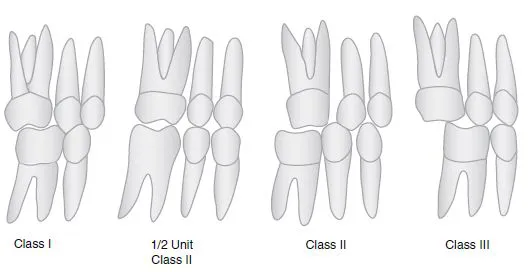
Buccal segment occlusion
The buccal segment occlusion (Figure 1.9):
- was devised by Edward Angle in 1890
- is still widely used today
- is based on the occlusion between the first permanent molar teeth, which erupt when the patient is about 6 years old
There are three classes:
- Class I – This is as near to the correct relationship as you see
- Class II – This is at least half a cusp width behind the ideal relationship
- Class III – This is at least half a cusp width in front of the ideal relationship
THE MIXED DENTITION
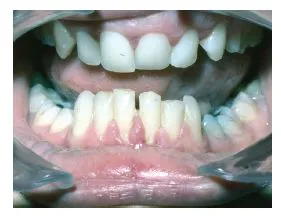
Sometimes parents see their child’s perfectly straight deciduous (baby) teeth fall out only to be replaced by a ‘jumble’ of crowded permanent teeth (Figure 1.10).
A combination of full-sized teeth in a face that still has a lot of growing to do often prompts parents to request an early orthodontic opinion. Permanent teeth can look huge in little faces.
The average times for permanent tooth eruption are:
- Age 6
- 1/1 lower central incisors
- 6/6 lower first molars
- 6/6 upper first molars
- Age 7
- 1/1 upper central incisors
- 2/2 lower lateral incisors
- Age 8
- 2/2 upper lateral incisors
- Age 11
- 3/3 lower canines (cuspids)
- 4/4 lower first premolars (bicuspids)
- 4/4 upper first premolars (bicuspids)
- Age 12
- 3/3 upper canines (cuspids)
- 5/5 lower second premolars (bicuspids)
- 5/5 upper second premolars (bicuspids)
- 7/7 upper second molars
- 7/7 lower second molars
- Age 18–25
- 8/8 upper third molars (wisdom teeth)
- 8/8 lower third molars (wisdom teeth)
Normally, patients begin orthodontic treatment between 10 and 13 years of age. At 10–11 years, they are still in the mixed dentition with:
- some deciduous teeth
- some permanent teeth
- some teeth yet to erupt
INDICATIONS FOR TREATMENT
Clinical indications for orthodontic treatment may be because the teeth:
- are overcrowded
- may have erupted out of position
- are protruding – Class II/1
- are in a reverse bite
- are in a self-damaging bite (Figure 1.11)
- are spaced
- are absent – hypodontia
- are damaged
Where there is a mild malocclusion, i.e.:
- with only very small irregularities
- where the tooth position does not compromise oral hygiene
- which does not interfere with function, e.g. biting off food, eating
orthodontic treatment may not be indicated, as it may not be seen to significantly improve dental health.
Those cases, e.g.:
- with overcrowded, protruding teeth
- with rotated teeth which make oral hygiene difficult and cause problems with caries (Figure 1.12)
- which visually deviate from average, e.g. a reverse bite
- which look unattractive and affect the smile
- which seriously affect function, e.g. makes chewing food difficult
are classed as malocclusions warranting treatment.
UNDERLYING CAUSES OF MALOCCLUSION OF THE TEETH
There may also be:
- underlying skeletal abnormalities
- facial asymmetries
These can be:
- hereditary (run in families, e.g. tendency to be Class III)
- a result of injury
- a result of illness affecting facial or skeletal growth
- a result of a syndrome or cleft
These may require orthodontic treatment as part of a multi-disciplinary care treatment pathway.
MULTI-DISCIPLINARY APPROACH
Some patients require orthodontic treatment in conjunction with other dental specialties.
These include:
- restorative (e.g. hypodontia patients needing implants/bridges or microdontia patients needing veneers or crowns)
- surgical (e.g. patients needing an osteotomy)
- cleft (e.g. patients needing alveolar bone grafting)
These patients have their orthodontic treatment in coordination with the o...