![]()
1
Surgical strategy
Learning objectives
To understand the principles of taking a clear history, performing an appropriate examination, presenting the findings and formulating a management plan for surgical diagnosis.
To understand the common nomenclature used in surgery.
Students on the surgical team, in dealing with their patients, should recognize the following steps in their patients’ management.
1 History taking. Listen carefully to the patient’s story.
2 Examination of the patient.
3 Writing notes.
4 Constructing a differential diagnosis. Ask the question ‘What diagnosis would best explain this clinical picture?’
5 Special investigations. Which laboratory and imaging tests are required to confirm or refute the clinical diagnosis?
6 Management. Decide on the management of the patient. Remember that this will include reassurance, relief of pain and, as far as possible, allaying the patient’s anxiety.
History and examination
The importance of developing clinical skills cannot be overemphasized. Excessive reliance on special investigations and extensive modern imaging (some of which may be quite painful and carry with them their own risks and complications) is to turn your back on the skills necessary to become a good clinician. Remember that the patient will be apprehensive and often will be in pain and discomfort. Attending to these is the first task of a good doctor.
The history
The history should be an accurate reflection of what the patient said, not your interpretation of it. Ask open questions such as ‘When were you last well?’ and ‘What happened next?’, rather than closed questions such as ‘Do you have chest pain?’. If you have a positive finding, do not leave the subject until you know everything there is to know about it. For example, ‘When did it start?’; ‘What makes it better and what makes it worse?’; ‘Where did it start and where did it go?’; ‘Did it come and go or was it constant?’. If the symptom is one characterized by bleeding, ask about what sort of blood, when, how much, were there clots, was it mixed in with food/ faeces, was it associated with pain? Remember that most patients come to see a surgeon because of pain or bleeding (Table 1.1). You need to be able to find out as much as you can about these presentations.
Keep in mind that the patient has no knowledge of anatomy. He might say ‘my stomach hurts’, but this may be due to lower chest or periumbilical pain – ask him to point to the site of the pain. Bear in mind that he may be pointing to a site of referred pain, and similarly do not accept ‘back pain’ without clarifying where in the back – the sacrum, or lumbar, thoracic or cervical spine, or possibly loin or subscapular regions. When referring to the shoulder tip, clarify whether the patient means the acromion; when referring to the shoulder blade, clarify whether this is the angle of the scapula. Such sites of pain may suggest referred pain from the diaphragm and gallbladder, respectively.
Table 1.1 Example of important facts to determine in patients with pain and rectal bleeding
| Exact site | Estimation of amount (often inaccurate) |
| Radiation | Timing of bleeding |
| Length of history | Colour – bright red, dark red, black |
| Periodicity | Accompanying symptoms – pain, vomiting (haematemesis) |
| Nature – constant/colicky | Associated shock – faintness, etc. |
| Severity | Blood mixed in stool, lying on surface, on paper, in toilet pan |
| Relieving and aggravating factors | |
| Accompanying features (e.g. jaundice, vomiting, haematuria) | |
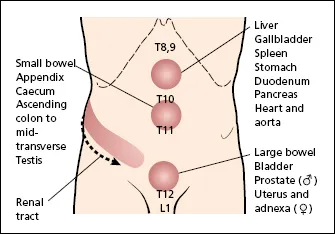
It is often useful to consider the viscera in terms of their embryology. Thus, epigastric pain is generally from foregut structures such as stomach, duodenum, liver, gallbladder, spleen and pancreas; periumbilical pain is midgut pain from small bowel and ascending colon, and includes the appendix; suprapubic pain is hindgut pain, originating in the colon, rectum and other structures of the cloaca such as the bladder, uterus and fallopian tubes (Figure 1.1). Testicular pain may also be periumbilical, reflecting the intra-abdominal origin of these organs before their descent into the scrotum – nev...