![]()
1
Neurology Worldwide: the Burden of Neurological Disease
Simon Shorvon
Neurological disease casts a heavy shadow on the lives of the patient, their family and friends and on society. The aim of all neurological services should be to alleviate the suffering associated with the disease, and to realize this aim the rational planning of such health services requires knowledge in four broad areas. First, information is required about the epidemiology of the condition – its frequency and distribution within a population, its causation, mortality and co-morbidity. Second, it is important to know the broad impact of the disease (the ‘burden of illness’) on individuals, families and on health services and societies and also its financial cost. Third, data are needed on the effectiveness (and cost-effectiveness) of diagnostic, investigatory and treatment interventions. Finally, knowledge is required of the existing health care resources and their distribution and priorities. The last two areas are outside the scope of this chapter, and here a necessarily extremely brief overview of selected issues related to the epidemiology and burden of illness is given, where possible using figures derived from studies from the National Hospital in London. These set the scene for the more detailed consideration of neurological disease contained in the rest of the volume.
Epidemiology of neurological disease
It is self-evident that knowledge of epidemiology will be important to underpin any decision about the provision of health care resources. It is also clear that epidemiological data (on frequency, distribution, mortality, etc.) are of little value unless related to an intervention or therapeutic advance. Epidemiclogical data is particularly valuable for resource provision. Sadly, however, in practice, even where reliable data exist, these are used only inconsistently in planning health care. It is for this reason that in many, indeed perhaps most, health care settings, the provision of facilities for neurological care is often surprisingly fragmented and inappropriately targeted.
Frequency and distribution of neurological disease
Incidence and prevalence are the most common measures of frequency used in medicine.
Incidence is defined as the rate at which new cases occur in a specified population during a specified period. The incidence rate is usually calculated as the number of new cases occurring per 100,000 of the general population per year.
Prevalence is defined as proportion of a population that are cases at a point in time. The prevalence rate is usually calculated as the number of existing cases per 1000 of the general population. Point prevalence is calculated as the number on a particular day (prevalence day) and period prevalence is calculated as the number in a population over a specified period of time. Lifetime prevalence is defined as the risk of acquiring the condition at any time during life and is another important figure.
For many neurological diseases, information on even these basic measures is incomplete. Furthermore, the frequency of many neurological disorders varies markedly in different geographical regions, differs in urban when compared with rural settings, may differ with ethnicity, and is of often linked to lifestyle and socio-economic factors.
In most neurological illnesses there are also striking differences in frequency at different ages, and so the age distribution of the population will affect the frequency, and some diseases have marked gender differences. For these reasons, age-specific or sex-specific rates, or frequency estimates in restricted age ranges, are generally more informative than crude rates. For instance, the annual incidence of stroke in a population is about 190/100,000/ year, but in the population over 65 years the rate is 1100/100,000/ year. Similarly, the incidence and prevalence of Parkinson’s disease in the general population is 20/100,000/year and 2/1000, and in those over 65 years is 160/100,000/year and 10/1000.
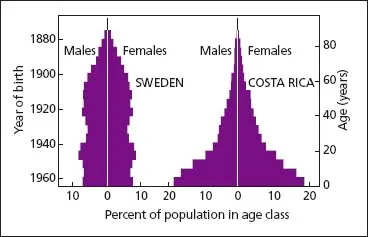
Changes in age structure in populations will impact heavily on the number of patients with diseases that have age-specificity. In most developing countries, the population has a far greater proportion of children and young adults than in developed countries (Figure 1.1 shows age structures in a typical developed [Sweden] and developing country [Costa Rica]). It is also important to recognize that although worldwide human populations are growing in an exponential fashion, growth rates vary widely among different countries and regions and the concept of ‘doubling time’ is a useful way of quantifying this. Doubling time – the time it is predicted to take for a population to double in size – depends not only on population size and mortality rates, but also on the number of children per woman (Table 1.1) and various other social and health parameters.
The approximate non-standardized figures for the prevalence and incidence of neurological disorders in a developed country are shown in Table 1.2. This table illustrates one other important point – that for chronic diseases, as for many neurological diseases, the incidence rates may be low but prevalence rates are high. This is important for health service planning, as the facilities required for incident cases are very different from prevalent cases. The former require provision for investigation and acute therapy and the latter largely for follow-up, social care, long-term therapy and rehabilitation.
The results of age-adjusted incidence and prevalence figures in a population of 100,230 persons in a selection of general practices served by the National Hospital for Neurology and Neurosurgery in London from a research project published in 2000 are shown in Tables 1.3–1.5. Here, the rates are adjusted for age to reflect the general UK population and are given alongside comparative results from other studies. Overall, the onset of 625 neurological disorders was observed per 100,000 population during the year of observation. Six per cent of the population in whom lifetime prevalence was surveyed had had a neurological disorder. In the UK, diseases of the nervous system accounted for 7.6% of all GP consultations between 1981 and 1982. The frequency of disability in private households amongst those over 16 years of age in the UK in 1971 was comprehensively delineat...