eBook - ePub
Pediatric Cardiovascular Medicine
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Pediatric Cardiovascular Medicine
About this book
The first edition of this text, edited by two of the world's most respected pediatric cardiologists, set the standard for a single-volume, clinically focused textbook on this subject. This new edition, revised and updated by contributors representing today's global thought leaders, offers increased coverage of the most important current topics, such as pediatric electrophysiology, congenital heart disease, cardiovascular genetics/genomics, and the identification and management of risk factors in children, while maintaining the clinical focus. Published with a companion website that features additional images for download, self-assessment questions designed to aid readers who are preparing for examinations, and other features, Pediatric Cardiovascular Medicine, Second Edition, is the perfect reference for residents, fellows, pediatricians, as well as specialists in pediatric cardiology.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Normal and Abnormal Cardiac Development
Introduction
In this chapter, the main events of cardiac morphogenesis are discussed. We focus on morphologic descriptions and insights based on the molecular biologic approaches in animal models that have enhanced and modified our understanding of normal and abnormal cardiac development, including relevance for adult disease with a developmental background.
Advances and limitations in studying human development
The normal cardiovascular development of the human embryo in its crucial stages from 2 to 8 weeks’ gestation has to be deduced from postmortem morphologic studies of abortion material [1]. In this category we are mainly dealing with spontaneous abortions and do not know whether the material reflects normal morphogenesis. Descriptions in the literature referring to normal and abnormal human development do not emphasize this aspect. An addition to early detection of human embryonic malformations, mainly providing information on disturbed genes and chromosomes, is provided by amniocentesis, chorionic villus biopsies, and subsequent FISH (fluorescent in situ hybridization) analysis with genetic markers. However, these are not examined within the first crucial 8 weeks of development. Fetal diagnosis is a rapidly expanding area with increasing technical possibilities of ultrasound and echo-Doppler investigations in utero. The earliest observations indicating normal or abnormal heart development refer to 11–12 weeks’ gestation [2]. Consequently, our knowledge of detailed cardiac morphogenesis relies on describing processes in animal species, the main embryonic models being avians (chick and quail) and rodents (mouse and rat) and more recently the zebrafish. With the development of transgenic techniques, the mouse embryo has become important, and we will regularly refer to mouse embryo models when discussing certain abnormalities of cardiac development.
Knowledge about an embryonic lethal phenotype after a gene knockout and the absence of a phenotype might contribute little to the understanding of human congenital cardiac malformations [3]; 85% of the diagnosed human cardiac malformations are described as having a multifactorial origin. Epigenetic, environmental, biomechanical, and hemodynamic factors have been underestimated in research on cardiogenic programming. Their role in the development of cardiac malformations has previously been acknowledged, however, and has led to the so-called mechanistic classification [4]. There are a few recent publications linking hemodynamics to cardiovascular developmental abnormalities [5–8], but their relation to gene expression and cardiogenic patterning is unclear. A multidisciplinary approach combining clinical knowledge with basic science will lead to new insights into developmental processes.
Formation of the cardiogenic plates and the cardiac tube
The cardiac developmental program starts with the formation within the splanchnic mesoderm of the bilateral cardiogenic plates, which give rise to the myocardium and probably to parts of the endocardium (Figure 1.1). The splanchnic mesoderm at the endoderm/mesoderm interface differentiates into the vascular endothelium [9] and part of the endocardium [10,11]. The evidence for a cardiogenic plate origin of the endocardium supports a dual origin for this layer of the heart [12].
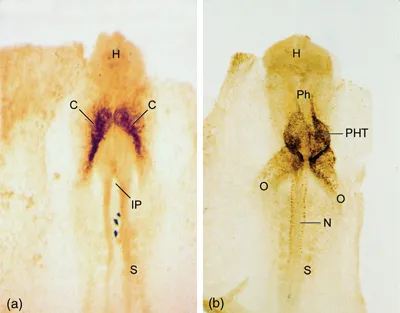
Figure 1.1 (a) Whole mount of a quail embryo (stage HH 8) viewed from the ventral aspect, showing the bilateral cardiogenic plates (C) that have not yet fused across the midline. At this stage, the staining is done by a nonspecific neurofilament antibody. (b) Whole mount of the fused primary heart tube (PHT) of a quail embryo (stage HH 10) viewed from the ventral aspect. The staining is by an anti-smooth muscle actin antibody, showing the myocardial lining of the tube. H, head region; IP, intestinal portal; N, neural tube; O, omphalomesenteric vein; Ph, pharyngeal region; S, somite. (Copyright Leiden University Medical Center.)
The bilateral asymmetric cardiogenic plates can be delineated early in embryonic life because several transcription factors and proteins are expressed. These expression patterns distinguish a first or primary heart field (PHF) laterally flanking the second heart field (SHF) component of the cardiogenic plate (Figure 1.2a). Whereas the first heart field differentiates, the secondary component remains part of the body wall mesoderm before its cells are recruited and incorporated into the poles of the cardiac tube. With formation of the cardiac tube, the pericardial coelomic cavity becomes continuous across the midline and the ventral mesocardium disappears. The cardiac tube is thereafter solely connected to the dorsal body wall or splanchnic mesoderm by the dorsal mesocardium that runs from the developing pharyngeal arches (arterial pole) to the sinus venosus (venous pole) (Figure 1.3). At this stage, the tube consists of an inner endocardial and an outer myocardial layer separated by cardiac jelly (Figures 1.2b and 1.3a).
Figure 1.2 Development of the heart from the first and second heart fields. (a) In the primitive plate, bilateral fields of cardiac mesoderm are present. Progenitor cells migrate from the primitive streak to the bilateral mesoderm (arrows). Cells depicted in yellow will contribute to the second heart field-derived parts of the heart, whereas cells depicted in brown depict the primary heart fields that will contribute the primary myocardial heart tube. (b) Schematic representation of the primary heart tube, consisting of endocardium and myocardium, with myocardial jelly between the two layers. Initially the primitive heart tube consists mainly of the AV canal and the LV. (c) After looping, several transitional zones can be distinguished in the tube, namely the sinoatrial transition (light blue, SAR) in between the sinus venosus and common atrium, the AV transition (dark blue, AVR) in between the common atrium and common ventricle, the primary fold (yellow, PF) in between the primitive right ventricle (RV) and LV, and a ventriculoarterial transitional (green, VAR) zone at the outflow tract (OT) of the heart. Second heart field-derived parts of the heart are depicted in yellow. (d) The heart after completion of atrial and ventricular septation. Due to outgrowth of the RV, a remodeling of the PF has occurred, and it has divided into a lateral septal part, the trabecula septomarginalis (TSM), that contains the right bundle branch [RBB, see (e)] and continues into the moderator band (MB). (e) Part of the transitional zones will contribute to definitive elements of the cardiac conduction system, depicted in red. Bright blue dots depict neural crest cells that contribute to the network of autonomic nerve fibers surrounding the sinoatrial node (SAN) and atrioventricular node (AVN). Shaded blue dots surrounding elements of the cardiac conduction system indicate neural crest cells with an inductive role in conduction system development. A, common atrium; AP, arterial pole; Ao, aorta; Ao sac, aortic sac; CV, cardinal vein; CS, coronary sinus; ICV, inferior caval vein; LA, left atrium; LAA, left atrial appendage; LBB, left bundle branch; LV, left ventricle; PT, pulmonary trunk; PV, pulmonary veins; RA, right atrium; RAA, right atrial appendage; SCV, superior caval vein; VP, venous pole. (Copyright Leiden University Medical Center.)
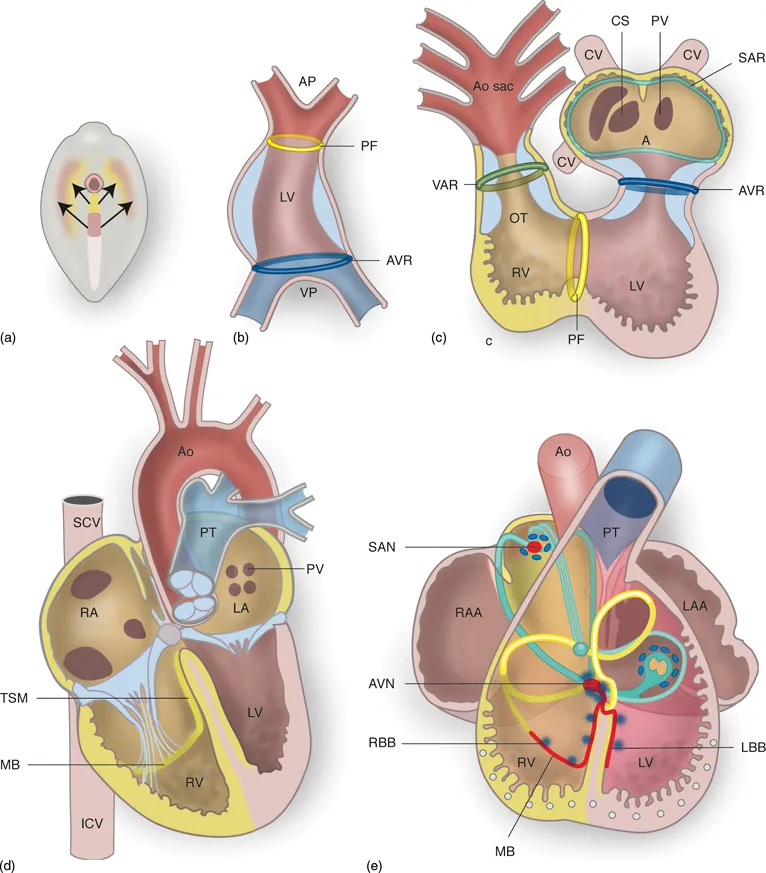
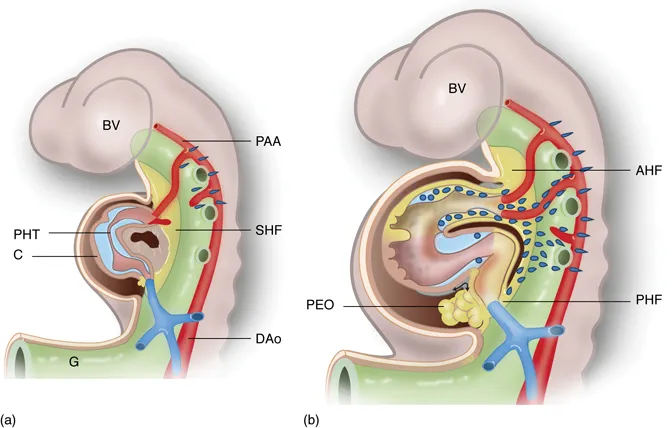
Figure 1.3 (a) Schematic representation of the primary heart tube (PHT, brown) after fusion of the bilateral plates of mesoderm. The tube is lined on the inside by cardiac jelly (blue). The mesoderm of the second heart field (SHF) is depicted by the yellow area behind the primary heart tube, and will during development contribute myocardium to both the arterial and venous poles of the heart [depicted by the yellow myocardium in (b)]. (b) The heart tube after contribution from the first and second heart fields have been made. The second heart field can be divided into the anterior heart field (AHF) and posterior heart field (PHF). The yellow lobulated structure that protrudes into the pericardial cavity at the venous pole of the heart is the pro-epicardial organ (PEO). Neural crest cells (depicted by blue dots) migrate from the neural crest along the arterial and venous pole into the heart. BV, brain ventricles; C, coelomic cavity; DAo, dorsal aorta; G, gut; PAA, pharyngeal arch arteries. (Copyright Leiden University Medical Center.)
Initially, the primitive cardiac endothelial network is remodeled into a single endocardial tube that connects the omphalomesenteric veins to the pharyngeal arch vasculature (Figure 1.1). The asymmetric cardiac jelly surrounding the endocardial tube suggests bilateral endocardial tubes, giving the wrong impression that two endocardial tubes have to fuse. From the onset, however, the endocardial tubes are connected by endocardial cells that cross the midline [13]. Real cardia bifida can occur spontaneously and can also be produced experimentally by retinoic acid overdose in the chicken embryo [14] or in a zebrafish mutational screen [15]. Therefore, each cardiogenic plate can potentially give rise to an independent cardiac tube, implying that fusion of the cardiogenic plates is unnecessary for the onset of cardiac formation. Nevertheless, cardia bifida is lethal to the embryo as further cardiac development is hampered and no connection with the endothelium of the pharyngeal vascular system is established.
Looping of the cardiac tube
The single cardiac tube is never completely straight as both cardiogenic plates have different dimensions [12]. Normally the cardiac tube loops to the right (D-loop) (Figure 1.2). Abnormalities in looping such as L-loop or anterior-loop formation are related to ventricular inversion, which differs from laterality problems as seen in abnormalities of the atrial situs.
The mechanisms underlying the looping direction are poorly understood, but several regulating genes have been described, such as sonic hedgehog, nodal and activin receptor IIa [16]. In mouse mutants iv/iv and inv, the laterality of the heart is also affected. The iv gene has been mapped to chromosome 12 in the mouse and is syntenic to chromosome 14q in the human. In the human, this abnormality is reflected in the heart by atrial isomerism and is discussed below when considering atrial development and septation.
During looping, the outflow tract becomes more ventrally positioned, moving in front of the atrioventricular (AV) canal. The arterial and venous poles remain fixed to the dorsal body wall (Figure 1.4 and Videoclip 1.1). Both remodeling of the inner curvature (site of the disruption of the dorsal mesocardium) and asymmetric addition of SHF-derived myocardium to the primary heart tube are essential for proper looping.
Contribution of first and second heart fields
Recent mouse studies, based on various transgenic mouse models with cell tracing [17–19], have shown that the primary heart tube does not contain all components necessary for the future mature heart [20]. The first heart field provides only for the AV canal and the future left ventricle (LV), implying that the primary heart tube already has additions of the second heart field (SHF) at both poles. The primary heart tube connects the omphalomesenteric veins at the venous pole via a small atrial component, the AV canal, and a primitive LV and small outflow tract component to the aort...
Table of contents
- Cover
- Series page
- Title page
- Copyright page
- Dedication
- List of Contributors
- Preface
- 1 Normal and Abnormal Cardiac Development
- 2 Genetics of Cardiovascular Disease in the Young
- 3 Developmental Physiology of the Circulation
- 4 Basic Anatomy and Physiology of the Heart, and Coronary and Peripheral Circulations
- 5 Pulmonary Vascular Pathophysiology
- 6 Clinical History and Physical Examination
- 7 Electrocardiography
- 8 Echocardiography
- 9 Radiographic Techniques
- 10 Cardiac Catheterization and Angiography
- 11 Exercise Testing
- 12 Thrombosis in Congenital and Acquired Disease
- 13 Genetic Testing
- 14 Practices in Congenital Cardiac Surgery: Pulmonary Artery Banding, Systemic to Pulmonary Artery Shunting, Cardiopulmonary Bypass, and Mechanical Ventricular Assist Devices
- 15 Postoperative Problems
- 16 Fetal Treatment
- 17 Newborn Diagnosis and Management
- 18 Noncardiac Problems of the Neonatal Period
- 19 The Epidemiology of Cardiovascular Malformations
- 20 Anatomy and Description of the Congenitally Malformed Heart
- 21 Atrial Level Shunts Including Partial Anomalous Pulmonary Venous Connection and Scimitar Syndrome
- 22 Atrioventricular Septal Defects
- 23 Ventricular Septal Defect
- 24 Aortopulmonary Shunts: Patent Ductus Arteriosus, Aortopulmonary Window, Aortic Origin of a Pulmonary Artery
- 25 Sinus of Valsalva Fistula
- 26 Systemic Arteriovenous Fistula
- 27 Left Ventricular Inflow Obstruction: Pulmonary Vein Stenosis, Cor Triatriatum, Supravalvar Mitral Ring, Mitral Valve Stenosis
- 28 Left Ventricular Inflow Regurgitation
- 29 Right Ventricular Inflow Obstruction
- 30 Left Ventricular Outflow Obstruction: Aortic Valve Stenosis, Subaortic Stenosis, Supravalvar Aortic Stenosis, and Bicuspid Aortic Valve
- 31 Left Ventricular Outflow Regurgitation and Aortoventricular Tunnel
- 32 Coarctation of the Aorta and Interrupted Aortic Arch
- 33 Right Ventricular Outflow Tract Obstruction
- 34 Total Anomalous Pulmonary Venous Connection
- 35 Tricuspid Atresia
- 36 Ebstein Anomaly of the Tricuspid Valve
- 37 Anomalies of the Coronary Sinus
- 38 Hypoplastic Left Heart Syndrome
- 39 Univentricular Heart
- 40 Pulmonary Atresia with Intact Ventricular Septum
- 41 Tetralogy of Fallot and Pulmonary Atresia with Ventricular Septal Defect
- 42 Complete Transposition of the Great Arteries
- 43 Congenitally Corrected Transposition of the Great Arteries
- 44 Transposition and Malposition of the Great Arteries with Ventricular Septal Defects
- 45 Common Arterial Trunk (Truncus Arteriosus)
- 46 Pulmonary Arteriovenous Malformations
- 47 Vascular Rings
- 48 Coronary Arterial Abnormalities and Diseases
- 49 Pulmonary Artery Sling
- 50 Abnormalities of Situs
- 51 Pediatric Pulmonary Hypertension
- 52 Central Nervous System Complications
- 53 Adults with Congenital Heart Disease
- 54 Quality of Life and Psychosocial Functioning in Adults with Congenital Heart Disease
- 55 Cardiac Arrhythmias: Diagnosis and Management
- 56 Syncope
- 57 Cardiovascular Disease, Sudden Cardiac Death, and Preparticipation Screening in Young Competitive Athletes
- 58 Cardiomyopathies
- 59 Pericardial Diseases
- 60 Infective Endocarditis
- 61 Rheumatic Fever
- 62 Rheumatic Heart Disease
- 63 Kawasaki Disease
- 64 Hypertension in Children and Adolescents
- 65 Cardiovascular Risk Factors: Obesity, Diabetes, and Lipids
- 66 Cardiac Tumors
- 67 Connective Tissue Disorders
- 68 Cardiac Involvement in the Mucopolysaccharide Disorders
- 69 Cardiovascular Manifestations of Pediatric Rheumatic Diseases
- 70 Pediatric Heart Transplantation
- 71 Cardiac Failure
- 72 Pediatric Cardiology in the Tropics and Underdeveloped Countries
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Pediatric Cardiovascular Medicine by James H. Moller, Julien I. E. Hoffman, James H. Moller,Julien I. E. Hoffman in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.