![]()
1
Thyroid
Hashimoto’s thyroiditis (chronic autoimmune thyroiditis)
Definition and epidemiology
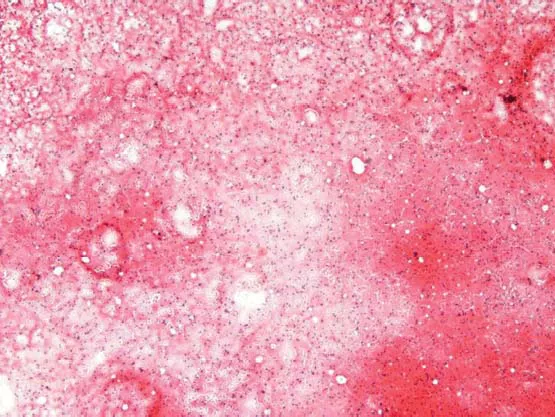
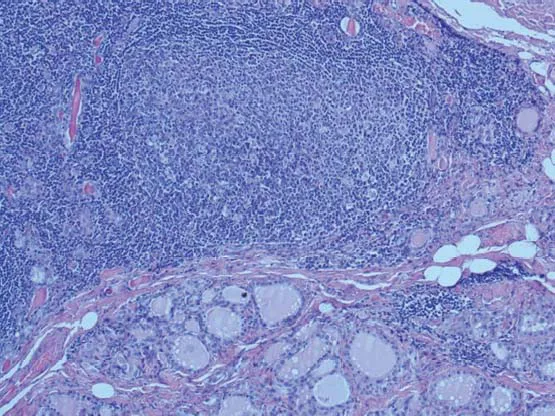
Hashimoto’s thyroiditis (HT), or chronic lymphocytic thyroiditis, is an autoimmune disease in which the thyroid gland is attacked by a variety of cell and antibody-mediated immune processes. The name “Hashimoto’s thyroiditis” is derived from the 1912 original report by Hashimoto describing patients with both goiter and intense lymphocytic infiltration of the thyroid (Figs 1.1 & 1.2) as “struma lymphomatosa.”
Hashimoto’s thyroiditis is the most common cause of primary hypothyroidism in iodine-sufficient areas of the world; it is among the most common causes of nonendemic goiter. On average 1.0–1.5/1000 people suffer from this disease. It occurs far more often in women than in men (incidence of 10 : 1 to 20 : 1, respectively), and it is most prevalent between 45 and 65 years of age. Occurrence in children is also uncommon, especially in populations where iodine is not a dietary scarcity.
Etiology and pathogenesis
Autoantibodies may be present against thyroid peroxidase, thyroglobulin, and thyroid-stimulating hormone (TSH) receptors, although a small percentage of patients may have none of these antibodies present. Antibody-dependent cell-mediated cytotoxicity is a substantial factor behind the apoptotic fallout of HT. Activation of cytotoxic T lymphocytes (CD8+ T cells) in response to cell-mediated immune response affected by helper T lymphocytes (CD4+ T cells) is central to thyrocyte destruction. Recruitment of macrophages is another effect of helper T-lymphocyte activation, with Th1-axis lymphocytes producing inflammatory cytokines within the thyroid tissue to further macrophage activation and migration into the thyroid gland for a direct effect. Infection, stress, sex steroids, pregnancy, iodine intake, and radiation exposure are known possible precipitating factors for HT. Fetal microchimerism within the maternal thyroid is also a possibility.
Signs and symptoms
Hashimoto’s thyroiditis very often results in hypothyroidism with bouts of hyperthyroidism. Symptoms of HT include weight gain, depression, mania, sensitivity to heat and cold, paresthesia, fatigue, panic attacks, bradycardia, tachycardia, high cholesterol, reactive hypoglycemia, constipation, migraine, muscle weakness, cramps, memory loss, infertility, hair loss, and myxedematous psychosis.
Diagnosis
Laboratory findings
Laboratory tests for HT include:
- Antithyroid peroxidase antibodies (TPOAbs) and thyroglobulin antibodies (TgAbs)
- TSH, free thyroxine (FT4)
- Total cholesterol, high density lipoprotein (HDL), and triglycerides
Imaging tests
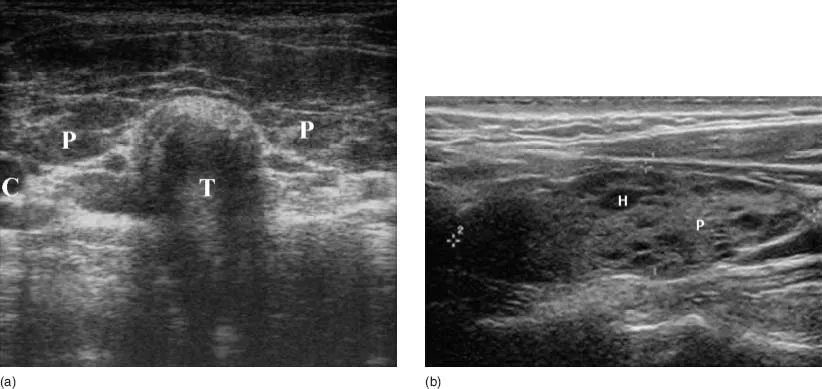
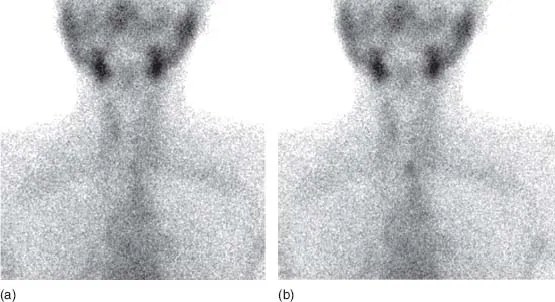
Imaging tests for HT include:
- Neck ultrasound (Fig. 1.3)
- Computed tomography (CT) scan (rare)
- 99mTcO4 thyroid scintigraphy (Fig. 1.4)
Treatment
In patients with primary hypothyroidism, the main treatment is levothyroxine.
Illustrations (Figs 1.1–1.4)
Graves’ disease (Basedow’s disease)
Definition and epidemiology
Graves’ disease (GD) is an autoimmune disease representing the most common cause of hyperthyroidism (60–90% of all cases).
Graves’ disease has a powerful hereditary component, affecting up to 2% of the female population, and is between five and ten times more common in females than in males (incidence of 5 : 1 to 10 : 1, respectively). It is also the most common cause of severe hyperthyroidism, which is accompanied by extended clinical signs and symptoms and laboratory abnormalities compared with milder forms of hyperthyroidism. About 30–50% of patients with GD will also suffer from Graves’ ophthalmopathy, which is caused by inflammation of the eye muscles mediated by an inflammatory immune process.
Etiology and pathogenesis
Graves’ disease is an autoimmune disorder in which the body produces antibodies to the receptor for thyroid stimulating hormone (TSHrAb). (Antibodies to thyroglobulin and thyroperoxidase may also be produced.) TSHrAb bind to the thyroid stimulating hormone (TSH) receptors, which are located on cells...