![]()
1
An introduction to drugs, their action and discovery
1.1 Introduction
The primary objective of medicinal chemistry is the design and discovery of new compounds that are suitable for use as drugs. This process involves a team of workers from a wide range of disciplines such as chemistry, biology, biochemistry, pharmacology, mathematics, medicine and computing, amongst others.
The discovery or design of a new drug not only requires a discovery or design process but also the synthesis of the drug, a method of administration, the development of tests and procedures to establish how it operates in the body and a safety assessment. Drug discovery may also require fundamental research into the biological and chemical nature of the diseased state. These and other aspects of drug design and discovery require input from specialists in many other fields and so medicinal chemists need to have an outline knowledge of the relevant aspects of these fields.
1.2 What are drugs and why do we need new ones?
Drugs are strictly defined as chemical substances that are used to prevent or cure diseases in humans, animals and plants. The activity of a drug is its pharmaceutical effect on the subject, for example, analgesic or β-blocker, whereas its potency is the quantitative nature of that effect. Unfortunately the term drug is also used by the media and the general public to describe the substances taken for their psychotic rather than medicinal effects. However, this does not mean that these substances cannot be used as drugs. Heroin, for example, is a very effective painkiller and is used as such in the form of diamorphine in terminal cancer cases.
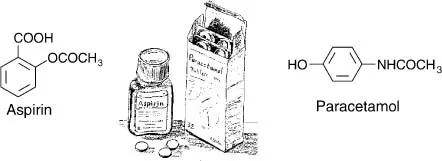
Drugs act by interfering with biological processes, so no drug is completely safe. All drugs, including those non-prescription drugs such as aspirin and paracetamol (Fig. 1.1) that are commonly available over the counter, act as poisons if taken in excess. For example, overdoses of paracetamol can causes coma and death. Furthermore, in addition to their beneficial effects most drugs have non-beneficial biological effects. Aspirin, which is commonly used to alleviate headaches, can also cause gastric irritation and occult bleeding in some people The non-beneficial effects of some drugs, such as cocaine and heroin, are so undesirable that the use of these drugs has to be strictly controlled by legislation. These unwanted effects are commonly referred to as side effects. However, side effects are not always non-beneficial; the term also includes biological effects that are beneficial to the patient. For example, the antihistamine promethazine is licenced for the treatment of hayfever but also induces drowsiness, which may aid sleep.
Drug resistance or tolerance (tachyphylaxis) occurs when a drug is no longer effective in controlling a medical condition. It arises in people for a variety of reasons. For example, the effectiveness of barbiturates often decreases with repeated use because the body develops mixed function oxidases in the liver that metabolise the drug, which reduces its effectiveness. The development of an enzyme that metabolises the drug is a relatively common reason for drug resistance. Another general reason for drug resistance is the downregulation of receptors (see section 8.6.1). Downregulation occurs when repeated stimulation of areceptor results in the receptor being broken down. This results in the drug being less effective because there are fewer receptors available for it to act on. However, downregulating has been utilised therapeutically in a number of cases. The continuous use of gonadotrophin releasing factor, for example, causes gonadotrophin receptors that control the menstrual cycle to be downregulated. This is why gonadotrophin-like drugs are used as contraceptives. Drug resistance may also be due to the appearance of a significantly high proportion of drug-resistant strains of microorganisms. These strains arise naturally and can rapidly multiply and become the currently predominant strain of that microorganism. Antimalarial drugs are proving less effective because of an increase in the proportion of drug-resistant strains of the malaria parasite.
New drugs are constantly required to combat drug resistance even though it can be minimised by the correct use of medicines by patients. They are also required for improving the treatment of existing diseases, the treatment of newly identified diseases and the production of safer drugs by the reduction or removal of adverse side effects.
1.3 Drug discovery and design: a historical outline
Since ancient times the peoples of the world have had a wide range of natural products that they use for medicinal purposes. These products, obtained from animal, vegetable and mineral sources, were sometimes very effective. However, many of the products were very toxic and it is interesting to note that the Greeks used the same word pharmakon for both poisons and medicinal products. Information about these ancient remedies was not readily available to users until the invention of the printing press in the fifteenth century. This led to the widespread publication and circulation of Herbals and Pharmacopoeias, which resulted in a rapid increase in the use, and misuse, of herbal and other remedies. Misuse of tartar emetic (antimony potassium tartrate) was the reason for its use being banned by the Paris parliament in 1566, probably the first recorded ban of its type. The usage of such remedies reached its height in the seventeenth century. However, improved communications between practitioners in the eighteenth and nineteenth centuries resulted in the progressive removal of preparations that were either ineffective or too toxic from Herbals and Pharmacopoeias. It also led to a more rational development of new drugs.
The early nineteenth century saw the extraction of pure substances from plant material. These substances were of consistent quality but only a few of the compounds isolated proved to be satisfactory as therapeutic agents. The majority were found to be too toxic although many, such as morphine and cocaine for example, were extensively prescribed by physicians.
The search to find less toxic medicines than those based on natural sources resulted in the introduction of synthetic substances as drugs in the late nineteenth century and their widespread use in the twentieth century. This development was based on the structures of known pharmacologically active compounds, now referred to as leads. The approach adopted by most nineteenth century workers was to synthesise structures related to that of the lead and test these compounds for the required activity. These lead-related compounds are now referred to as analogues.
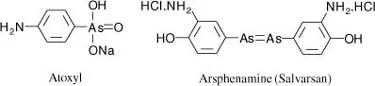
The first rational development of synthetic drugs was carried out by Paul Ehrlich and Sacachiro Hata who produced arsphenamine in 1910 by combining synthesis with reliable biological screening and evaluation procedures. Ehrlich, at the beginning of the nineteenth century, had recognised that both the beneficial and toxic properties of a drug were important to its evaluation. He realised that the more effective drugs showed a greater selectivity for the target microorganism than its host. Consequently, to compare the effectiveness of different compounds, he expressed a drug’s selectivity and hence its effectiveness in terms of its chemotherapeutic index, which he defined as:
At the start of the nineteenth century Ehrlich was looking for a safer antiprotozoal agent with which to treat syphilis than the then currently used atoxyl. He and Hata tested and catalogued in terms of his therapeutic index over 600 structurally related arsenic compounds. This led to their discovery in 1909 that arsphenamine (Salvarsan) could cure mice infected with syphilis. This drug was found to be effective in humans but had to be used with extreme care as it was very toxic. However, it was used up to the mid- 1940s when it was replaced by penicillin.
Ehrlich’s method of approach is still one of the basic techniques used to design and evaluate new drugs in medicinal chemistry. However, his chemotherapeutic index has been updated to take into account the variability of individuals and is now defined as its reciprocal, the therapeutic index or ratio:
where LD50 is the lethal dose required to kill 50 per cent of the test animals and ED50 is the dose producing an effective therapeutic response in 50 per cent of the test animals. In theory, the larger a drug’s therapeutic index, the greater is its margin of safety. However, because of the nature of the data used in their derivation, therapeutic index values can only be used as a limited guide to the relative usefulness of different compounds.
The term structure–activity relationship (SAR) is now used to describe Ehrlich’s approach to drug discovery, which consisted of synthesising and testing a series of structurally related compounds (see Chapter 3). Although attempts to quantitatively relate chemical structure to biological action were first initiated in the nineteenth century, it was not until the 1960s that Hansch and Fujita devised a method that successfully incorporated quantitative measurements into structure–activity relationship determinations (see section 3.4.4). The technique is referred to as QSAR (quantitative structure–activity relationship). QSAR methods have subsequently been expanded by a number of other workers. One of the most successful uses of QSAR has been in the development in the 1970s of the antiulcer agents cimetidine and ranitidine. Both SAR and QSAR are important parts of the foundations of medicinal chemistry.
At the same time as Ehrlich was investigating the use of arsenical drugs to treat syphilis, John Langley formulated his theory of receptive substances. In 1905 Langley proposed that so-called receptive substances in the body could accept either a stimulating compound, which would cause a biological response, or a non-stimulating compound, which would prevent a biological response. These ideas have been developed by subsequent workers and the theory of receptors has become one of the fundamental concepts of medicinal chemistry. Receptor sites (see Chapter 8) usually take the form of pockets, grooves or other cavities in the surface of certain proteins and glycoproteins in the living organism. They should not be confused with active sites (see section 9.3), which are the regions of enzymes where metabolic chemical reactions occur. It is now accepted that the binding of a chemical agent, referred to as a ligand (see section 8.1), to a receptor sets in motion a series of biochemical events that result in a biological or p...