![]()
Chapter 1
Introduction to Lung Cancer and Mesothelioma
Alison Leary
Key points
- Lung cancer is the most common cause of cancer worldwide and the most common cause of cancer death in the UK.
- The causes of lung cancer are multifactorial but there is a strong and established link with tobacco. Increasingly women who are never smokers are being diagnosed with lung cancer.
- Despite high levels of service improvement in cancer, there remains variability in the level of care provided to people with lung cancer.
Introduction
Malignant disease of the lung is a rare condition. The Middlesex Hospital Reports show only 890 cases of cancer of the Lung, 317 found at post mortem examination since records began…. As for prognosis a fatal termination is inevitable with average duration of the disease [life expectancy] to be 13.2 months.
Fowler and Rickman (1898), Diseases of the Lung
Lung cancer is currently the most common form of cancer worldwide…life expectancy is usually between three to seven months from diagnosis.
From Boyle et al. (2000), Textbook of Lung Cancer
From being a virtually unknown disease at the end of the nineteenth century, lung cancer has become the most common worldwide cancer. In just over 100 years lung cancer has become a modern epidemic. Thought to account for over 3 000 000 deaths each year worldwide and 33 400 deaths in the UK from the 39 000 diagnosed (Cancer Research UK (CRUK) 2010a) and with a 5-year survival rate of only 8–11% overall.
Five-year survival from lung cancer has barely improved in the last 30 years (Spiro and Silvestri 2005) but there has been a decline in deaths in the male population and an increase in female deaths. In contrast, 1-year survival has improved to some degree. In England and Wales 1-year survival in men with advanced non-small-cell lung cancer (NSCLC) rose from 15% in the 1970s to 25% in 2000/2001 (Coleman et al. 2004).
Average 5-year survival in the UK is 8.95%, which can be broken down by country:
- England (8.6%)
- Scotland (8.0%)
- Northern Ireland (10.2%)
- Wales (9.0%)
This is compared with 12.3% average in Europe (Berrino et al. 2007) and 15% in the USA (Reis et al. 2004). Surgical resection of lung cancer is the primary management, but the vast majority of patients with lung cancer present at a stage that is too advanced for surgery. Surgical resection rates are lower in the UK (11%) than Europe (17%) and North America (21%) (CRUK 2010a).
It is hoped that development of targeted therapies, earlier detection and increased opportunity for surgical intervention may improve the survival rate in lung cancer.
Epidemiology and causes of lung cancer
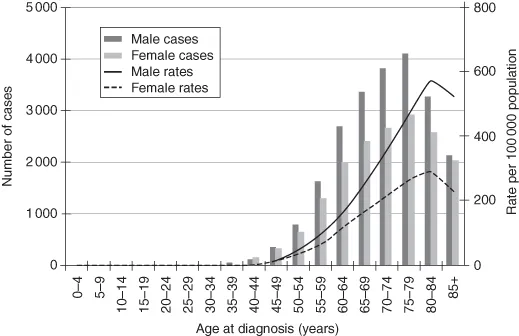
Until recently – as late as the 1990s – lung cancer was the most frequently occurring cancer in the UK. It has now been overtaken by breast cancer but is still the cause of 1 in 7 of all new cancer cases and 1 in 5 cancer deaths. In 2007, 39 473 people were diagnosed with lung cancer (CRUK 2010b). Most cases of lung cancer (approximately 86%) occur in people over the age of 60 years; the peaking age is 75–84 years (Fig. 1.1). Lung cancer accounts for 15% of all new male cancers and 12% of all new female cancers in the UK (CRUK 2010b). Lifetime risk of developing lung cancer is 1 in 14 for men and 1 in 21 for women in the UK.
Lung cancer incidence and social deprivation
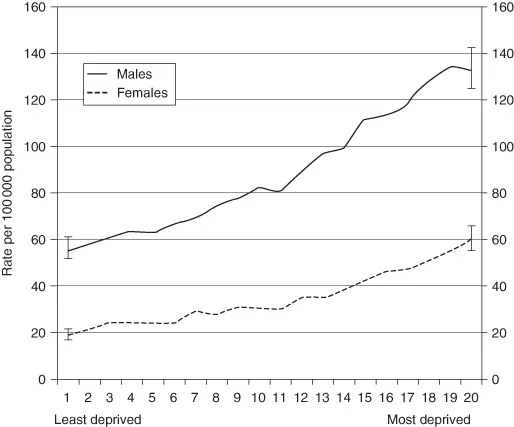
Higher incidence of lung cancer has also been linked to areas associated with higher economic deprivation. Data from the 1990s shows that the incidence of lung cancer was thought to be three times higher in women in deprived areas and 2.5 times higher in men compared with the least-deprived areas (Fig. 1.2).
Lung cancer remains a cancer prevalent in areas of socioeconomic deprivation. Data from the National Cancer Intelligence Network (NCIN) in 2008 on the years 2000–2004 demonstrated that if the incidence of lung cancer were the same in the most deprived groups as in the least deprived this would account for 11 250 fewer cases of lung per year (NCIN 2008). Rates of lung cancer in Scotland are among the highest in the world, reflecting the history of high smoking prevalence. Many authors now comment that lung cancer is endemic in society (Boyle et al. 2000). The increase in incidence of lung cancer in the last hundred years has certainly been recognised. One of the causes of this rise is the now axiomatic link with smoking, particularly of tobacco.
Lung cancer incidence and smoking
From the mid-1950s there was an increase in the understanding of the aetiology of lung cancer and also the growing awareness that lung cancer was becoming more prevalent, reaffirming a causal link to smoking tobacco. This was in part due to the benchmark studies of Doll and Hill (1950, 1952, 1954). The body of evidence was so strong that in the USA the surgeon general was moved to produce an official statement on smoking and health that caused a worldwide reaction. After the publication of these documents, a more descriptive epidemiology of lung cancer occurred with the publishing of large cohort studies, for example the work of the National Cancer Institute in the USA.
From the 1960s onwards more epidemiological research into the rise of smoking-related diseases, of which non-small-cell lung cancer is just one, also charted the way in which smoking habits have changed. For example, in the 1970s consumers were made aware of tar levels and encouraged to smoke low-tar products. Some authors contend that this merely seems to have changed the histological subtype of lung cancer without reducing its incidence. Although tobacco smoking is thought to account for the majority of lung cancer deaths (CRUK 2010b) some authors, particularly from studies in the United States, cite as many as 10–20% of all newly diagnosed lung cancers being in those who have never smoked (never-smokers).
The link between lung cancer and smoking established in the 1950s and subsequent health promotion campaigns have influenced the public perception of lung cancer as a disease of smokers. In a recent survey by the UK Lung Cancer Coalition it was found that 40% of the population considered lung cancer to be a self-inflicted cancer, despite the fact that 1 in 8 lung cancer patients are never-smokers. The belief that lung cancer was a self inflicted cancer was higher (50%) in higher socioeconomic groups and lower (35%) in lower socioeconomic groups (UK Lung Cancer Coalition (UKLCC) 2005), and so whereas other patients with cancer are seen as victims by society, patients with lung cancer are seen as at least partly culpable for their disease. This then affects their perception of their own disease and some authors contend that lack of investment in research and other areas of lung cancer care stem from the less vocal nature of the lung cancer population and that as a group lung cancer patients tend to come from lower socioeconomic backgrounds with more limited access to education. Previous educational background influences how the cancer is perceived by the patient and family and also influences the subsequent information needs of the patient (Chapple et al. 2004; Jacobs-Lawson et al. 2009) Because of the established epidemiological link with tobacco use, lung cancer patients often experience feelings of stigmatisation and guilt (Chapple et al. 2004), which gives an added dimension to their suffering.
Lung cancer incidence and ethnicity
Data recently published by the National Cancer Intelligence Network on cancer incidence by survival in major ethnic group illustrates the difficulty of looking at ethnicity incidence. Data in this area is limited as it is only in recent years that routine data on ethnicity has been collected. However, from these data we can see that the rate of lung cancer in all non-white ethnic groups is significantly lower than in the white ethnic group, with people of all ages ranging from 23.1 to 37.2 per 100 000 in the Asian ethnic group, from 30.1 to 48.9 per 100 000 in the black ethnic group, from 22.4 to 48.6 per 100 000 in the Chinese ethnic group, and from 21.9 to 43.1 per 100 000 in the mixed ethnic group. In the white ethnic group the rate was 61.1 to 62.6 per 100 000 (NCIN 2009).
A standardised relative survival for the Asian ethnic group was significantly higher than the white ethnic group, for both 1 and 3 years; there is no significant difference in a standardised relative survival between black and white ethnic groups. For males aged 15–64 years at diagnosis, relative survival for the Asian ethnic group was significantly higher than for the white ethnic group at both 1 and 3 years. Given that the majority of lung cancers occur after the age of 60, these data have to be viewed in that context. For males aged 65–99 years, relative survival was significantly higher than in the white ethnic group for both Asian and black ethnic groups at both 1 and 3 years.
The causes of lung cancer
Although the link between smoking and lung cancer was established in the 1950s, the smoking or direct consumption of tobacco-related products is thought not to be the sole cause of lung cancer. It is estimated that exposure to passive smoking in the home causes around 11 000 deaths every year in the UK, from not only lung cancer but also stroke and ischaemic heart disease (CRUK 2010b).
Other causes of lung cancer are thought to include radon gas, which is a naturally occurring gas that increases the chance of developing lung cancer, particularly among smokers. Radon is present throughout the UK, but in some areas geological conditio...