![]()
1
Anatomy
Learning objective
To learn the anatomy of the eye, the orbit and the third, fourth and sixth cranial nerves, to permit an understanding of medical conditions affecting these structures.
Introduction
A knowledge of ocular anatomy and function is important to the understanding of eye diseases. A brief outline is given below.
Gross anatomy
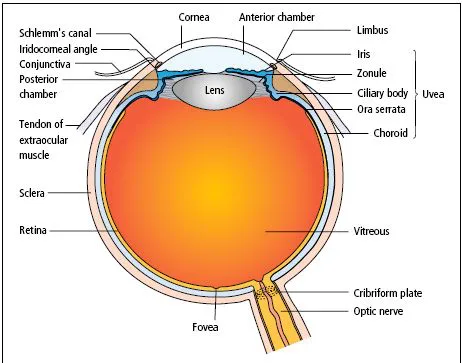
The eye (Figure 1.1) comprises:
- A tough outer coat which is transparent anteriorly (thecornea) and opaque posteriorly (the sclera). The junction between them is called the limbus. The extraocular muscles attach to the outer sclera while the optic nerve leaves the globe posteriorly.
- A rich vascular coat (the uvea) forms the choroid posteriorly and the ciliary body and iris anteriorly. The choroid lines the retina, to which it is firmly attached and nourishes its outer two-thirds.
- The ciliary body contains the smooth ciliary muscle, whose contraction allows the lens to take up a more curved shape which permits focusing for near objects. The ciliary epithelium secretes aqueous humour and maintains the ocular pressure. The ciliary body provides attachment for the iris, which forms the pupillary diaphragm.
- The lens lies behind the iris, supported by the zonular fibrils, which run from the lens equator to the ciliary body. When the eye is focused for distance, tension in the zonule maintains a flattened profile of the lens.
- The cornea anteriorly and the iris and central lens posteriorly form the ante- rior chamber, whose periphery is the iridocorneal angle or drainage angle. The angle is lined by a meshwork of cells and collagen beams called the trabecular meshwork, through which aqueous drains into Schlemm’s canal and thence into the venous system via the aqueous veins. This is the basis of aqueous drainage.
- Between the iris, lens and ciliary body lies the posterior chamber, a narrow space distinct from the vitreous body. Both the anterior and posterior chambers are filled with aqueous humour. Between the lens and the retina lies the vitreous body, occupying most of the posterior segment of the eye.
Anteriorly, the bulbar conjunctiva of the globe is reflected from the sclera into the fornices and thence onto the posterior surface of the lids where it forms the tarsal conjunctiva. A connective tissue layer (Tenon’s capsule) separates the conjunctiva from the sclera and is prolonged backwards as a sheath around the rectus muscles.
The orbit
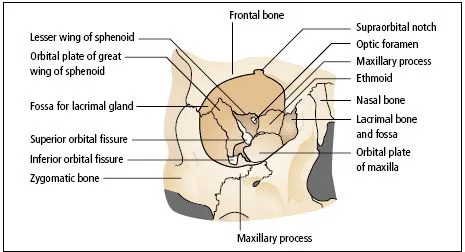
The eye lies within the bony orbit, which has the shape of a four-sided pyramid (Figure 1.2). At its posterior apex is the optic canal, which transmits the optic nerve to the chiasm, tract and lateral geniculate body. The superior and inferior orbital fissures allow the passage of blood vessels and cranial nerves which supply orbital structures. The lacrimal gland lies anteriorly in the superolateral aspect of the orbit. On the anterior medial wall lies the fossa for the lacrimal sac.
The eyelids (tarsal plates)
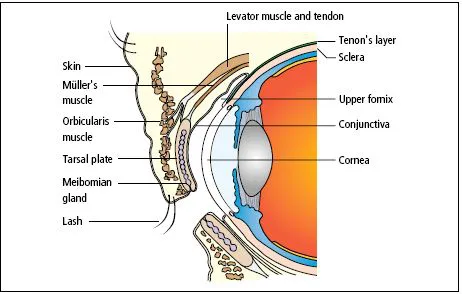
The eyelids (Figure 1.3):
- offer mechanical protection to the anterior globe;
- spread the tear film over the conjunctiva and cornea with each blink;
- contain the meibomian oil glands, which provide the lipid component of the tear film;
- through closure and blinking prevent drying of the eyes;
- contain the puncta through which the tears flow into the lacrimal drainage system.
They comprise:
- an anterior layer of skin;
- the orbicularis muscle, innervated by the seventh nerve;
- a tough collagenous layer (thetarsal plate) which houses the oil glands;
- an epithelial lining, the tarsal conjunctiva, which is reflected onto the globe via the fornices.
Contraction of the peripheral fibres of the orbicularis muscle results in a protective, forced eye closure, while that of the inner, palpebral muscle results in the blink.
The levator muscle passes forwards to the upper lid and inserts by an aponeurosis into the tarsal plate. It is innervated by the third nerve. Damage to the nerve or weakening of the aponeurosis in old age results in drooping of the eyelid (ptosis). A flat, smooth muscle, innervated by the sympathetic nervous system, arises from the deep surface of the levator and inserts into the tarsal plate. If the sympathetic supply is damaged, a slight ptosis results (Horner’s syndrome).
The meibomian oil glands deliver their oil to the skin of the lid margin, just anterior to the mucocutaneous junction. This oil spreads onto the anterior surface of the tear film with each blink, to form a lipid layer which retards evaporation. Far medially on the lid margins, two puncta form the initial part of the lacrimal drainage system.
The lacrimal drainage system
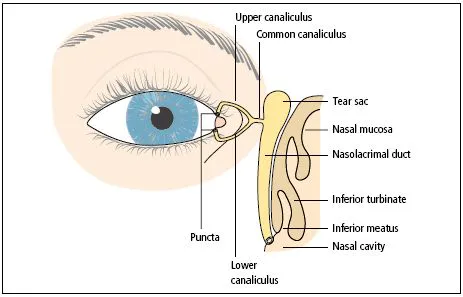
Tears drain into the upper and lower puncta and then into the lacrimal sac via the upper and lower canaliculi (Figure 1.4). They form a common canaliculus before entering the lacrimal sac. The nasolacrimal duct passes from the sac to the nose. Failure of the distal part of the nasolacrimal duct to fully canalize at birth is the usual cause of a watering, sticky eye in an infant. Tear drainage is an active process. Each blink helps to pump tears through the system.
Detailed functional anatomy
The tear film
The ocular surface is bathed constantly by the tears, secreted mainly by the lacrimal gland but supplemented by conjunctival secretions. They drain away via the nasolacrimal system.
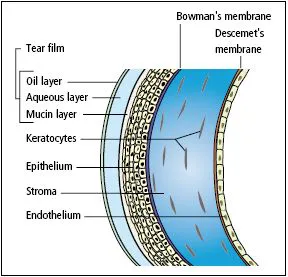
The epithelial cells of the ocular surface express a mucin glycocalyx which renders the surface wettable. When the eyes are open, the exposed ocular surface (the cornea and exposed wedges of bulbar conjunctiva) are covered by a tear film, 3 µm thick. This comprises three layers:
1 a mucin gel layer produced by the conjunctival goblet cells, in contact with the ocular surface;
2 an aqueous layer produced by the lacrimal gland;
3 a surface oil layer produced by the meibomian glands and delivered to the lid margins.
Functions of the tear film
- It provides a smooth air/tear interface for distortion-free refraction of light at the cornea.
- It transmits oxygen to the avascular cornea.
- It removes debris and foreign particles from the ocular surface through the flow of tears.
- It has antibacterial properties through the action of lysozyme, lactoferrin, defensins and the immunoglobulins, particularly secretory IgA.
The tear film is replenished with each blink.
The cornea
The cornea (Figure 1.5) is 0.5 mm thick and comprises:
- The epithelium, an anterior non-keratinized squamous layer, thickened peripherally at the limbus where it is continuous with the conjunctiva. The limbus houses the germinative stem cells of the corneal epithelium.
- An underlying stroma of collagen fibrils, ground substance and fibroblasts. The regular packing, small diameter and narrow separation of the collagen fibrils account for corneal transparency. This orderly architecture is maintained by regulating stromal hydration.
- The endothelium, a monolayer of non-regenerating cells which actively pump ions and water from the stroma, controlling corneal hydration and hence transparency.
The difference between the regenerative capacity of the epithelium and endothelium is important. Damage to the epithelial layer, by an abrasion for example, is rapidly repaired by cell spreading and proliferation. Endothelial damage, by disease or surgery, is repaired by cell spreading alone, with a loss of cell density. A point is reached when loss of its barrier and pumping functions leads to over - hydration (oedema), disruption of the regular packing of its stromal collagen and corneal clouding.7
The nutrition of the cornea is supplied almost entirely by the aqueous humour, which circulates through the anterior chamber and bathes the poste- rior surface of the cornea. The aqueous also supplies oxygen to the posterior stroma, while the anterior stroma receives its oxygen from the ambient air. The oxygen supply to the anterior cornea is reduced but still sufficient during lid closure, but a too -tightly fitting contact lens may deprive the anterior cornea of oxygen and cause corneal, especially epithelial, oedema.
Functions of the cornea
- It protects the internal ocular structures.
- Together with the lens, it refracts and focuses light onto the retina. The junction between the ambient air and the curved surface of the cornea, covered by its optically smooth tear film, forms a powerful refractive interface.
The sclera
- The sclera is formed from interwoven collagen fibrils of different widths lying within a ground substance and maintained by fibroblasts.
- It is of variable thickness, 1 mm around the optic nerve head and 0.3 mm just posterior to the muscle insertions.
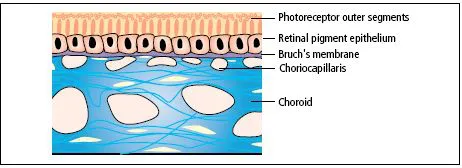
The choroid
- The choroid (Figure 1.6) is formed of arterioles, venules and a dense, fenestrated capillary network.
- It is loosely attached to the sclera.
- It has a remarkably high blood flow.
- It nourishes the deep, outer layers of the retina and may have a role in its temperature homeostasis.
- Its basement membrane, together with that of the retinal pigment epithelium (RPE), forms the acellular Bruch’s membrane, which acts as a diffusion barrier between the choroid and the retina.
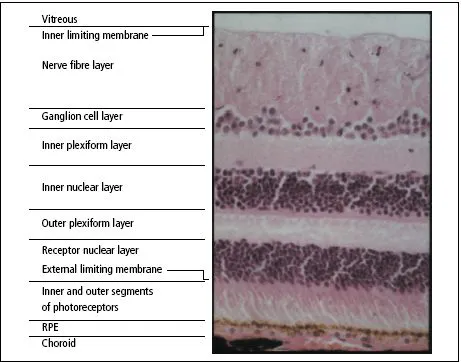
The retina
The retina (Figure 1.7) is a highly complex structure derived embryologically from the primitive optic cup. Its outermost layer is the...