Following the familiar, easy-to-use
at a Glance format, and in full-colour, this brand new title provides an accessible introduction and revision aid for medical students and junior doctors. Reflecting the increased profile of Emergency Medicine in clinical practice and the medical school curriculum,
Adult Emergency Medicine at a Glance provides a user-friendly overview of the key subjects that will enable any student or junior doctor to 'hit the ground running' when they enter one of the most exciting areas of clinical medicine.
Adult Emergency Medicine at a Glance is:
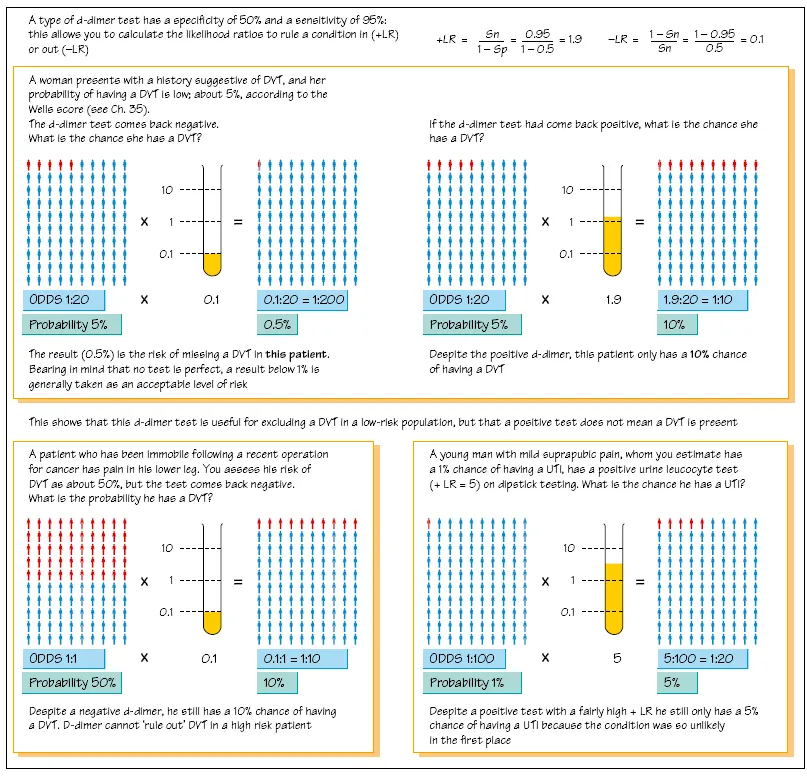
- A concise, visually orientated course in emergency medicine that is perfect for both study and revision
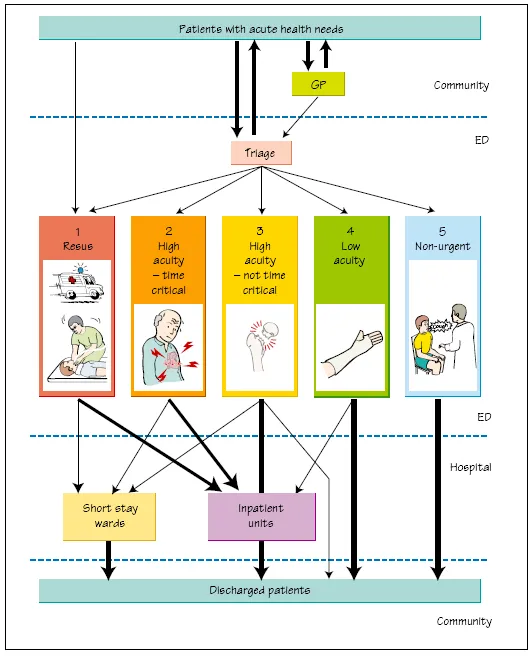
- Organised around symptoms: 'Short of Breath', rather than diagnoses: 'Pneumonia'
- Focused on the most common or dangerous conditions you will see in the Emergency Department and includes the latest cardiac resuscitation guidelines
- Comprehensively illustrated throughout with over 47 full-page colour illustrations