eBook - ePub
Revisiting Cardiac Anatomy
A Computed-Tomography-Based Atlas and Reference
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This new atlas represents a fresh fresh approach to cardiac anatomy, providing images of unparalleled quality, along with explanatory text, to show in vivo heart anatomy and explain the clinically relevant underlying anatomic concepts. In spite of amazing proliferation of information on the Internet and multiple websites filled with up-to-date information, there is no similarly detailed and systematic compilation of morphological imaging with CT. Organized for both systematic learning and to serve as a quick, yet detailed reference for specific clinical questions, this book is an invaluable resource for medical students and residents, cardiologists, and especially surgeons, interventionalists and electrophysiologists, who depend on ever more detailed imaging support in order to successfully perform increasingly complex coronary and noncoronary structural interventions and other procedures.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Anatomy of the Heart for a Dissector
Introduction
This chapter provides a general description of the heart anatomy and offers an outline of the relevant clinical information. Images are produced using state of the art multidetector scanner on living subjects and by meticulous dissection techniques on cadaveric specimens. Detailed discussions on specific anatomic locations are presented in the subsequent chapters.
Heart Orientation within the Thorax
Generally, cross-sectional imaging study of the heart requires reconstruction of two groups of imaging planes including body and heart planes. Standard body planes include three orthogonal cuts in axial (transverse), coronal, and sagittal orientations. Heart planes also include three orthogonal planes in relation to the heart axes [1, 2]. Short-axis images, which correspond to the plane of the atrioventricular (AV) groove, are oblique and are oriented closer to the vertical than to the horizontal plane. Horizontal long-axis (four-chamber) views are double oblique planes perpendicular to both the interventricular septum and the AV plane of the heart. Vertical long-axis (two-chamber) views of the heart are parallel to the interventricular septum (Figure 1.1).
Everyone must be familiar with radiographic borders of the heart in different projections (Figure 1.2). On anterior projection, the right cardiac border is formed by the right atrium (RA), while the left cardiac border is formed by the left ventricle (LV). The right ventricle (RV) and the left atrium (LA) are superimposed structures and are not border-forming, and additional projections are required to review them. Diaphragmatic surface is formed by the RV. On the lateral projection, the anterior cardiac border is the RV, while the posterior cardiac border is composed of both the LV and the LA.
Anteriorly, the heart is covered by the sternum and the costal cartilages. The heart has an extensive diaphragmatic surface inferiorly (Figure 1.3). Posteriorly, the heart lies on the esophagus and the tracheal bifurcation, and bronchi that extend into the lung. The sternum lies anteriorly and provides rigid protection to the heart during blunt trauma.
The true posterior surface of the heart is commonly termed the base of the heart, which is formed largely by the LA. The term “base of the heart” is not frequently used and is restricted to the “origin of the great vessels.” The inferior surface of the heart is also closely related to the diaphragm and should not be entirely called posterior. In supine position, along with elevation of the diaphragm, the lower surface of the heart largely faces inferiorly; however, in upright position, with full inspiration, the heart stands vertically and these walls face posteroinferiorly [1]. Because of the obliquity of the surfaces of the ventricles, the diaphragmatic surface of the RV is truly inferior and the diaphragmatic wall of the LV faces posteroinferiorly (Figures 1.3–1.5).
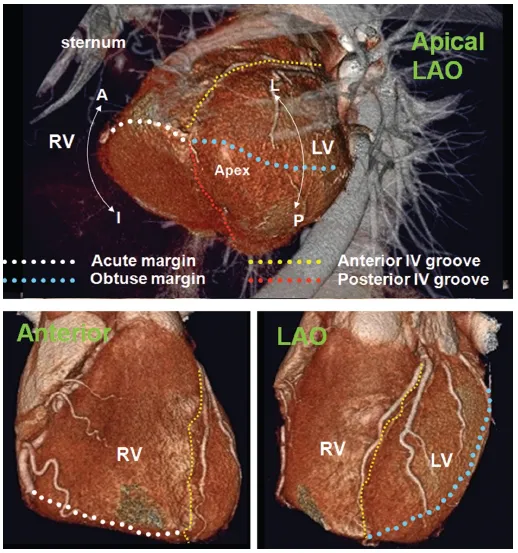
The heart is a three-sided pyramid located in the middle mediastinum. When viewed from its apex, the three sides of the ventricular mass are readily seen (Figure 1.5). Two of the edges are named. The acute margin lies inferiorly and describes a sharp angle between the sternocostal and diaphragmatic surfaces. The obtuse margin lies superiorly and is much more diffuse. The posterior margin is unnamed but is also diffuse in its transition.
The Right Atrium
The RA is the chamber of the heart that receives systemic venous blood return from the superior vena cava (SVC) and inferior vena cava (IVC) and coronary venous return from the coronary sinus. Looking at three-dimensional images of the heart from the top, RA is positioned to the right and anteriorly, while the LA is situated to the left and mainly posteriorly [3] (Figure 1.6)
Figure 1.1 Standard body (a) versus heart planes (b). The heart may be viewed in three standard anatomic planes: transaxial (Ax), coronal (Cor), and sagittal (Sag). The three major planes of the heart include short axis (SAX), horizontal long axis (four chamber, 4ch), and vertical long axis (two chamber, 2ch). Although these planes are perpendicular to one another, the body planes transect the heart obliquely, while the heart planes transect the body obliquely.
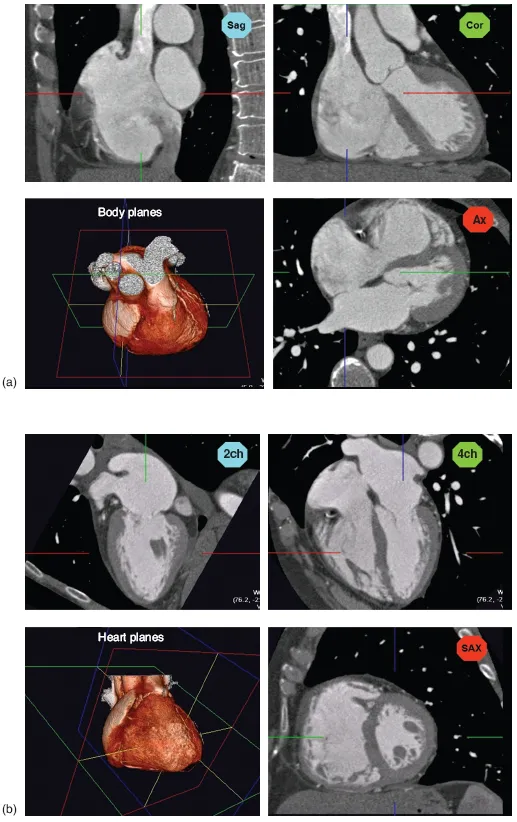
Figure 1.2 Radiographic projections are shown. All images are obtained with a 64-slice MDCT with three-dimensional reconstruction. Postprocessing is performed to show the relationship of the heart to the thoracic cage. Angiographic projections show the relation of the coronary arteries to the cardiac chambers. LAO, left anterior oblique projection; RAO, right anterior oblique projection.
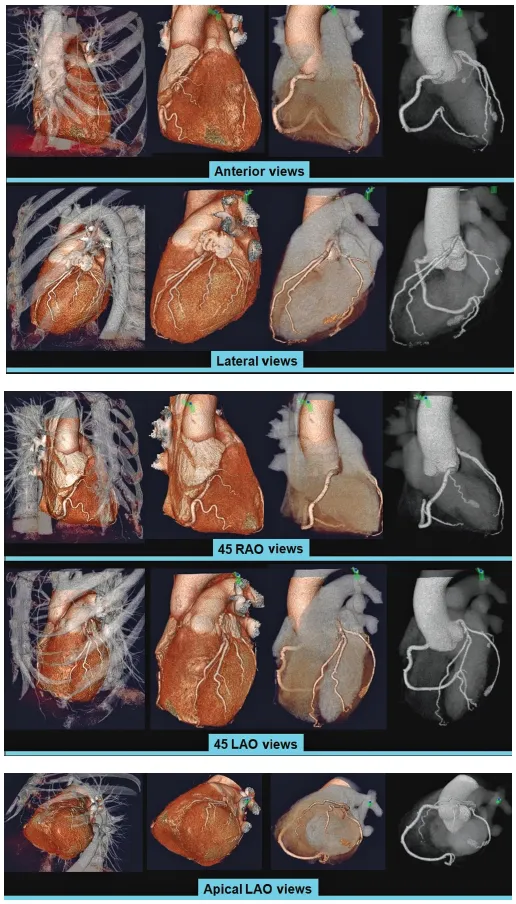
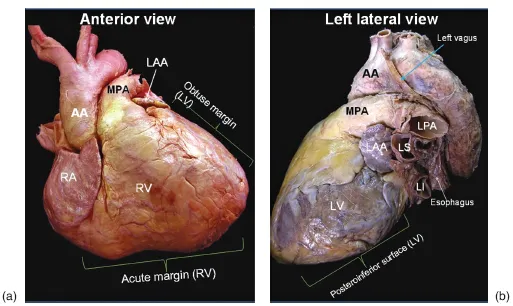
Figure 1.3 Ventricular margins and surfaces of cadaveric heart photographed in attitudinal positions to simulate the views as seen in living condition. (a) Anterior view and (b) Left lateral view of the heart. AA, ascending aorta; LAA, left atrial appendage; LPA, left pulmonary artery; LS and LI, left superior and left inferior pulmonary veins; LV, left ventricle; MPA, main pulmonary artery; RA, right atrium; RV, right ventricle.
From a spatial point of view, the RA may be divided into lateral, medial, inferior, and posterior walls. The RA comprises three components: the appendage, the venous part (sinus venarum), and the vestibule [4, 5]. One of morphologic characteristics of the RA is the presence of the crista terminalis. This C-shaped muscular ridge separates the smooth-walled sinus venarum from the trabeculated appendage (the right half of the primitive atrium) [6]. The crista terminalis varies in size and extent in different individuals (Figure 1.7; see also Chapter 9, cardiac anatomy for electrophysiologic interventions). Another indicator of the right atrial morphology is a large, wide-based appendage (Figure 1.6). Some anatomists define the appendage as the anterosuperior protrusion of the body of the RA, an anatomic feature rather than an anatomic subdivision. The vestibule, also known as supravalvular lamina, is a smooth muscular rim surrounding the tricuspid orifice [1] (Figure 1.8). The pectinate muscles do not reach this area (Figure 1.5; see also Chapter 9). The right coronary artery (RCA) runs in the epicardial fat next to the vestibule.
Terminal groove is a fat-filled sulcus on epicardial side, which corresponds internally to crista terminalis (Figure 1.6, the right lateral view). The sinus node and terminal segment of sinoatrial (SA) node artery are located in this groove, close to the superior cavoatrial junction.
Figure 1.4 CT angiography views. The ventricular surfaces are shown is relation to the thorax (body) and the heart itself. A, anterior; dotted yellow line, interventricular groove; L, lateral; LV, left ventricle; P, posterior; RV, right ventricle.
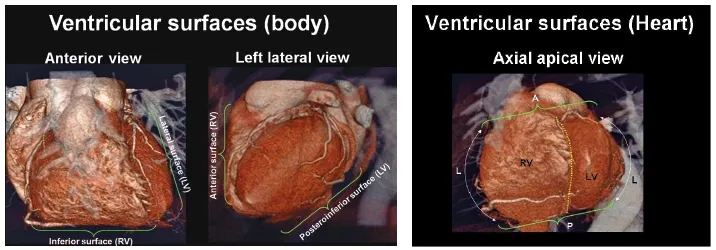
Figure 1.5 The margins of the heart. The acute margin is applied to the right ventricle (RV) only between the sternocostal (A, anterior) and diaphragmatic (I, inferior) surfaces. In an anterior view, the acute margin forms the lower border and the right atrium forms the right lateral border of the heart. The term “obtuse margin” denotes the posterolateral aspect of the left ventricle and atrium. It is defined as the junction between the lateral (L) and posterior (P) walls of the left ventricle (LV). In left anterior oblique (LAO) projection view, it forms the left border of the heart. Obtuse margin is a critical anatomic landmark, and in many instances, an artery (obtuse marginal, a branch of the LCx artery) runs along it.
The sinus venarum is mainly located in the posterolateral wall of the RA between the SVC and IVC orifices [7] (Figure 1.6). From the third week after the development of the primitive heart tube, the primitive atria are separated from the sinus venosus by a segmentation termed the SA ring. The sinus venosus has two horns. The right horn gives rise to all the intercaval regions of the RA including the crista terminalis, the Eustachian ridge, and the Thebesian valve (Figure 1.6). The left horn gives rise to the coronary sinus [8]. The interatrial septum is located posteromedially.
The RA is home to important parts of the cardiac conduction system including the SA and the AV nodes (AVNs) [9–11]. The SA node (SAN) is a banana-shaped structure in the subepicardial side of superior cavoatrial junction, composed of cells slightly smaller than normal working cells (Figure 1.11; see also Chapters 9). It is the source of the cardiac impulse. Because of the vicinity of the sinus node to the epicardial surface, it may be damaged in selected cardiac surgeries or extensive pericardial diseases [9]. The SAN is supplied by the SAN artery. The SAN artery is usually, a single branch, arising from the proximal RCA (60%) or the left circumflex (LCx) artery (40%) (see Chapter 4 and 9 for details). In the majority of hearts, the SAN artery passes through the center of SAN [11] (Figure 1.9).
The AVN is located within the boundaries of Koch’s triangle near its apex. The triangle of Koch is an important anatomic landmark of the RA, which is commonly used for electrophysiologic studies (Figure 1.17; see also Chapter 9). This triangle is bordered posteriorly by the tendon of Todaro (fibrous extension from the Eustachian valve), anteriorly by the septal leaflet of the tricuspid valve, and inferiorly by the ostium of the coronary sinus (Figure 1.10). The size of Koch’s triangle is variable in different individuals. The apex of this triangle corresponds to the central fibrous body of the heart [12].
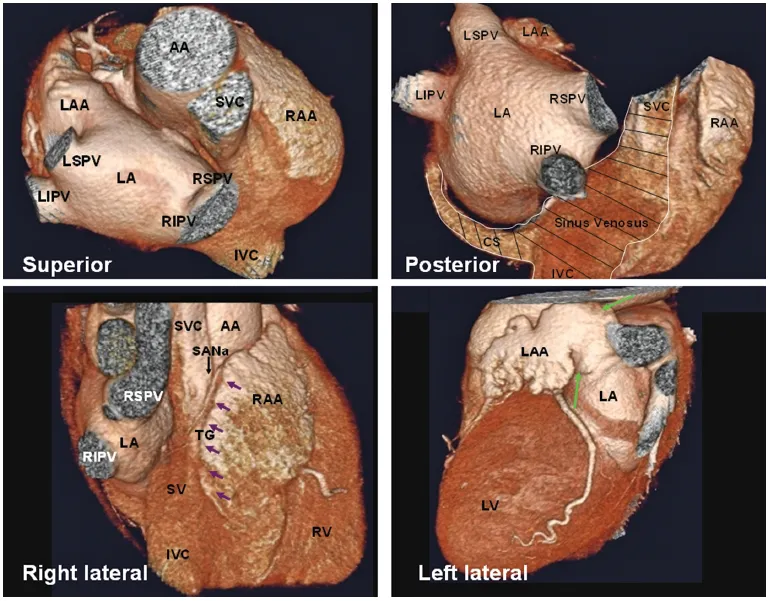
Figure 1.6 Atrial epicardial views. When viewed from the top (superior), the cavity of the right atrium is positioned to the right and anterior, while the left atrium is situated to the left and mainly posteriorly. On the posterior view, the anatomic boundaries of structures arising from the sinus venosus (SV) of the right atrium are shown (shaded area). Lower images are right and left lateral views of the heart. The dominant feature on the right side is a large, triangular shaped, atrial appendage. Terminal groove (TG) is between sinus venosus and RAA (small arrows). Note the sinoatrial node (SAN) artery running in this groove. The left atrial appendage (LAA) is a small lobulated structure. It is a potential site for deposition of thrombus owing to its trabeculated margin and narrow neck (green arrows). AA, ascending aorta; CS, coronary sinus; IVC, inferior vena cava; LA, left atrium; LIPV, left inferior pulmonary vein; LSPV, left superior pulmonary vein; LV, left ventricle; RA, right atrium; RAA, right atrial appendage; RIPV, right inferior pulmonary vein; RSPV, right superior pulmonary vein; SANa, sinoatrial node artery; SVC, superior vena cava. (Reprinted from Saremi and Krishnan [3], with permission.)
The AVN consists of a compact portion and an area of transitional cells. The compact portion lies over the central fibrous body [13] (Figure 1.19; see also Chapter 9). The AVN continues distally with the penetrating bundle of His. The AVN artery originates from the distal RCA (80–90%) and penetrates into the base of the posterior interatrial septum (inferior pyramidal space) at the level of crux of the heart in 80–87% of patients (Figure 1.11). In the remaining, it originates from the distal LCx artery [14–16].
The inferior wall of the RA is a complex area with several important anatomic landmarks [7,17]. The IVC and the coronary sinus connect to this portion of the RA. The Eustachian valve guards the anterior margin of the IVC. It is usually membranous and variably developed (Figure 1.26; see also Chapter 9). It may look fenestrated or contain muscles. Usually it inserts medially to the Eustachian ridge or sinus septum, which is the border between the oval fossa and the coronary sinus. The medial border of the Eustachian valve continues as a tendon of Todaro that runs in the musculature of the Eustachian ridge. Mistakenly, the valve may be sutured to the anterior rim of an atrial septal defect at the time of shunt repair. Laterally, the Eustachian valve merges into the crista terminalis. In some cases, it is large, posing an obstacle to pass a catheter.
Figure 1.7 Crista terminalis (CT) is a fibromuscular ridge formed by the junction of the sinus venosus and primitive right atrium (red arrows). The entire CT lies between the pectinate muscles and the sinus venarum. The origin of the crest at the interatrial groove is confluent with the origin of another important muscular fascicle, Bachmann bundle (yellow arrows). The crest arches anterior to the orifice of the SVC (precaval band) and extends to the area of the anterior interatrial groove. The parasagittal band (PB, blue arrows) or septum spurium is a large pectinate muscle arising from the precaval portion of the crest. It divides the right atrial appendage into medial and lateral compartments. The inferior border of the CT near the IVC orifice is unclear. It breaks up into a series of trabeculations in the area of the atrial wall known as the cavotricuspid isthmus. AA, ascending aorta; BB, Bachmann bundle; IVC, inferior vena cava; LA, left atrium; RA, right atrium; RAA, right atrial appendage; SVC, superior vena cava.
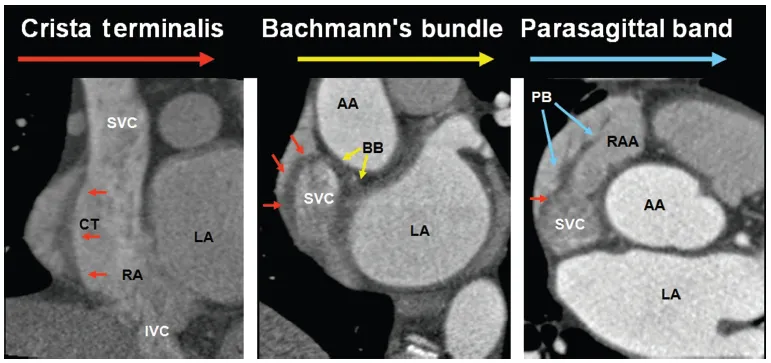
Figure 1.8 The right atrial vestibule, also known as supravalvular lamina, is a smooth muscular rim surrounding the tricuspid orifice (green arrows). The pectinate muscles do not reach this area. The right coronary artery runs in epicardial fat next t...
Table of contents
- Cover
- Title Page
- Copyright
- List of Contributors
- Preface
- 1: Anatomy of the Heart for a Dissector
- 2: Anatomical and Pathophysiological Classification of Congenital Heart Disease
- 3: CT in Pediatric Heart Disease
- 4: Mitral and Aortic Valves Anatomy for Surgeons and Interventionalists
- 5: Clinical Applications of CT Imaging of the Aortic and Mitral Valves
- 6: Computed Tomography for Percutaneous Aortic Valve Replacement
- 7: Mitral Valve Disease Imaging
- 8: The Aortic Root
- 9: Coronary Anatomy for Interventionalists
- 10: Coronary Anatomy for Surgeons
- 11: Anatomy for Electrophysiologic Interventions
- 12: Coronary Atherosclerosis: CT Imaging for the Preventive Cardiologist
- 13: Nomograms for Coronary Computed Tomographic Angiography
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Revisiting Cardiac Anatomy by Farhood Saremi in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.