The most complete, up-to-date reference on antigen retrieval and immunohistochemistry
An antigen is a substance that prompts the generation of antibodies and can cause an immune response. The antigen retrieval (AR) technique is in wide use across the globe, and is a critical technique used in medical diagnosis of disease, particularly clinical targeted cancer treatment.
Antigen Retrieval Immunohistochemistry Based Research and Diagnostics discusses several scientific approaches to the standardization of quantifiable immunohistochemistry (IHC). Based on the development and application of AR by the editors, this volume summarizes recent achievements in AR-IHC and analyzes numerous cutting-edge issues for future research projects.
Featuring contributions from a worldwide group of leading experts and research scientists in the field, this important work:
Summarizes the key problems in the four fields of antigen retrieval
Discusses the advances of AR techniques and their applications
Provides practical methods and protocols in AR-IHC, such as extraction of nucleic acids and proteins for molecular analysis, cell/tissue sample preparation, and standardization and development of various techniques to meet the future needs of clinical and research molecular analysis
Encourages further research in AR and IHC, particularly how AR methods might be employed for improved test performance and the development of greater reliability and reproducibility of IHC
Includes an appendix of related laboratory protocols
Antigen Retrieval Immunohistochemistry Based Research and Diagnostics is intended for clinical pathologists, molecular cell biologists, basic research scientists, technicians, and graduate students who undertake tissue/cell morphologic and molecular analysis and wish to use and extend the power of immunohistochemistry. It is also pertinent for most biotechnology companies majoring in development of IHC products.
Wiley Series in Biomedical Engineering and Multi-Disciplinary Integrated Systems / Kai Chang, Series Editor
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Part I: RECENT ADVANCES IN ANTIGEN RETRIEVAL TECHNIQUES AND ITS APPLICATION
CHAPTER 1
STANDARDIZATION OF ANTIGEN RETRIEVAL TECHNIQUES BASED ON THE TEST BATTERY APPROACH
SHAN-RONG SHI and CLIVE R. TAYLOR
Following the development of the antigen retrieval (AR) technique in 1991,1 hundreds of articles have been published worldwide that document its application in immunohistochemistry (IHC) for archival formalin-fixed, paraffin-embedded (FFPE) tissue sections. In addition, there are numerous articles that focus on standardization of the AR technique, stimulated by the current demand for a more quantitative method of IHC.2–6 The critical importance of standardization of antigen retrieval immunohistochemistry (AR-IHC) has been emphasized by the American Society of Clinical Oncology and the College of American Pathologists in their Guideline Recommendations for human epidermal growth factor receptor 2 (HER2) testing in breast cancer.7 The problem was, however, recognized and addressed to some degree much earlier. To optimize the results of AR-IHC in formalin paraffin sections, a “test battery” approach was proposed in 1996.8 The basic principle of this approach is based on the fact that two major factors influence the achievement of a satisfactory result of AR-IHC, namely, the heating condition (heating temperature × heating time) and the pH value of the AR solution (in which the FFPE tissue sections are immersed during heating).8–12 In practice, it suffices to test the (new) primary antibody using three different pH values, ranging from low (acidic), moderate (neutral), and high (basic) buffer solutions (or other comparable commercial AR solutions) under three heating temperatures: low (below boiling), moderate (boiling), and high (pressure cooker or autoclave), to establish an optimal AR protocol for tested antibodies (Table 1.1). Subsequently, numerous investigators have demonstrated the advantages of using this simple test battery method. As emphasized by O’Leary,2 the use of a “test battery” provides a rapid way to optimize AR for a particular antibody/antigen pair.
TABLE 1.1 Test Battery Suggested for Screening an Optimal Antigen Retrieval Protocol
a One more slide may be used for control without AR treatment. Citrate buffer of pH 6.0 may be used to replace Tris–HCl buffer, pH 7.0–8.0, as the results are the same.
b The temperature of super-high at 120°C may be reached by either autoclaving or microwave heating at a longer time.
c The temperature of mid-high at 90°C may be obtained by either a water bath or a microwave oven monitored with a thermometer.
Reprinted with permission from Shi et al., J. Histochem. Cytochem. 1997; 45: 327–343.
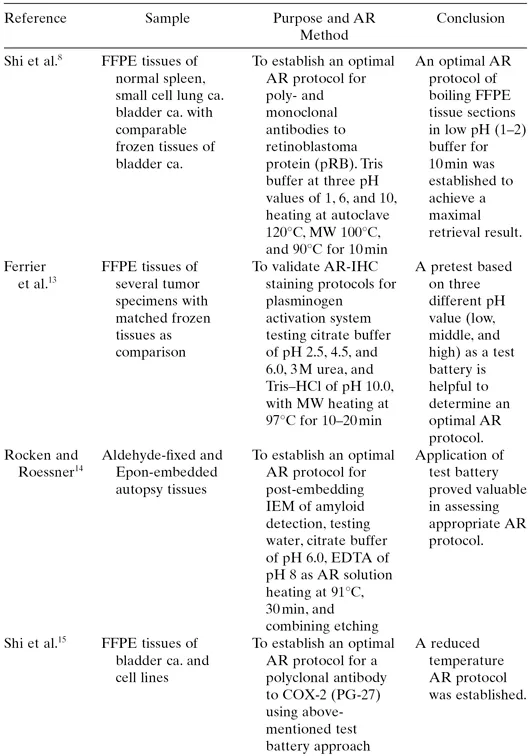
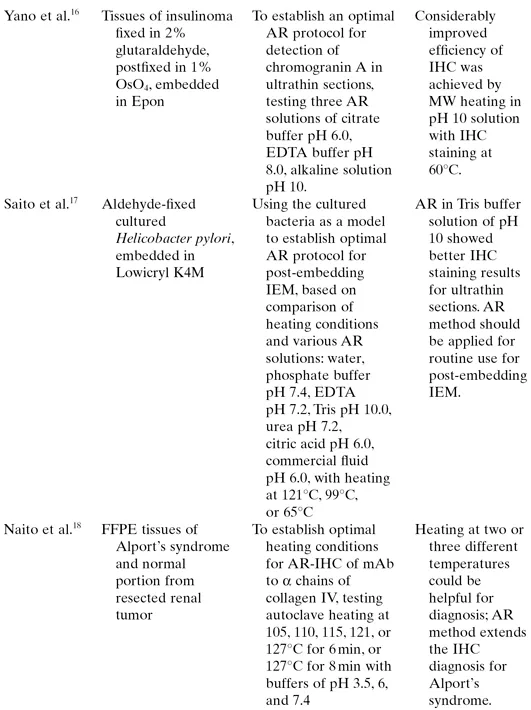
Recent studies have further extended the application of this approach to establish and validate the optimal AR protocol for various antibodies (exemplified in Table 1.2) with different detection systems, employing a multi-tissue microarray (TMA) to achieve a rapid and accurate evaluation.26,27 It has become apparent that significant differences can be found in IHC staining results among various primary antibodies and different detection systems with the use of different AR protocols. For example, Pan et al.27 evaluated the consistency of IHC staining for four antibodies to thyroid transcription factor (TTF)-1, manufactured by Dako, Zymed, Novocastra, and Santa Cruz, employing TMA blocks of 77 hepatocellular carcinomas and 334 nonhepatic epithelial tumors, using two solutions for AR treatment. Significantly different cytoplasmic IHC staining results were observed among different antibodies, as well as different AR solutions (e.g., Dako Target Retrieval Solution vs. ethylenediaminetetraacetic acid [EDTA] buffer at pH 8.0). In another study, Gill et al.21 standardized an AR method for IHC staining using antibody to a neuronal nuclear protein, NeuN, as the outcome measure. They compared three different pH values of AR solutions including low, middle, and high pH, with heating at three temperatures of 95, 100, or 105°C, for 15 or 20 min. They found that heating FFPE tissue sections in an alkaline pH buffer at high temperature gave the best results. The utility of the test battery approach used to establish optimal AR protocols has been demonstrated by abundant literature as summarized in Table 1.2.
TABLE 1.2 Randomly Selected Examples of Test Battery Approach Documented in Abundant Literature
Note: All tissue samples are human source unless otherwise noticed.
Ca., carcinoma; MW, microwave.
The increasing attention directed to the adverse effects of variation in sample preparation upon the quality of IHC staining of FFPE tissues has served to reinforce the importance of determining the optimal AR method for each antibody/detection system/antigen to achieve optimal retrieval and optimal staining of tissues that may have been processed and stored in different and unknown ways (see Chapter 5 for details). Practically, in considering the busy workload in a clinical service laboratory, we recommend a two-step procedure based on the typical design of a test battery (Table 1.1): in the first step, test three AR solutions at different pH values under one heating condition (100°C for 10 min) to find the optimal pH value; in the second step, test optimal heating conditions based on the optimal pH identified in step 1.28 Similarly, Hsi29 recommended using microwave pressure cooker as the standard heating condition for testing two commonly used AR solutions, citrate buffer of pH 6.0 and EDTA solution at pH 8.0, along with protease digestion. With the goal of identifying the optimal AR protocol for a new primary antibody, they used five different concentrations of the antibody, including the manufacturer’s recommended dilution, plus two serial twofold dilutions above and below this concentration. As seen in Table 1.2, many investigators have already accepted the basic principle of test battery, incorporating three levels of pH values and three heating conditions (Table 1.1). However, within this model, different investigators have used different heating methods and different AR methods to achieve optimal results for their individual laboratories. With this broad variety of approaches, clearly, we are a long way from achieving a universal method, even if such is possible.
1.1 SEARCHING FOR NOVEL CHEMICAL SOLUTIONS
Namimatsu et al.30 reported a novel AR solution containing 0.05% citraconic anhydride, pH 7.4, for heating FFPE tissue sections at 98°C for 45 min. They compared the IHC staining results using 62 commonly used antibodies and other conventional AR protocols (0.01 M citrate buffer, pH 6.0 in a pressure cooker; or 0.1 M Tris–HCl buffer containing 5% urea, pH 9.0 microwave heating for 10 min), and found that most antibodies showed stronger intensity with the new method. In particular, some difficult-to-detect antigens such as CD4, cyclin D1, granzyme β, bcl-6, and CD25 gave distinct IHC staining signals only by using the new protocol, leading to a claim that the method might be a candidate for the “universal” approach.
We therefore tested Namimatsu’s protocol and also obtained satisfactory results.31 Among 30 antibodies tested, more than half (53%) showed a stronger intensity of IHC when using the citraconic anhydride for AR, as compared to citric acid buffer, whereas 12 antibodies (43%) gave equivalent results. There was only one antibody (OC-125) that, in our hands, gave a stronger intensity using conventional citric buffer for AR. When using citraconic anhydride for AR, the heating conditions of boiling (100°C) or less than boiling (98°C) temperature yielded identical results for most antibodies tested (90%). However, 3 of 30 antibodies showed lower intensity at 100°C. In addition, some antibodies showed nonspecific background staining at 100°C. In particular, we demonstrated that when using antibody to retinoblastoma protein (pRB), the new protocol had advantages over a previously published low pH protocol,8 including superior morphologic preservation, greater reproducibility, and more intense staining signal.
As a further motivation, there is evidence that establishing the optimal AR protocol will also contribute to standardization of IHC, through “equalizing” variable IHC staining results obtained following different times of formalin fixation. In the light of the studies described above, further studies were conducted as to the utility of the citraconic anhydride method.
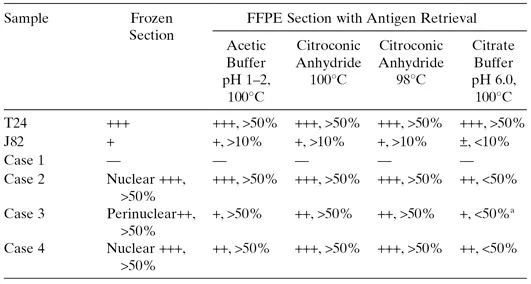
First Step: A comparative study of IHC staining for pRB was carried out using paired sections of frozen versus FFPE cell/tissue samples, comparing citraconic anhydride as the AR solution under two different temperatures (98oC vs. 100oC), with solutions of low pH buffer (acetate buffer, pH 1–2) and citrate buffer (pH 6.0). Findings are summarized in Table 1.3. Conventional citrate buffer yielded inconsistent and weaker signals for all specimens, except the cell line T24 (Table 1.3, Fig. 1.1). Stronger intensity was found in pRB-positive cases, while using the citraconic anhydride for AR (Fig. 1.1), although more nonspecific background staining was observed using citraconic anhydride under boiling condition (Fig. 1.1, C vs. D, and R vs. S).
TABLE 1.3 Comparison of pRB-IHC between Frozen and Paraffin Sections Using Four Protocols of AR
Notes: T24 and J82 are cell lines of bladder cancer. Cases 1 to 4 are specimens of human bladder cancer.
a Although peripheral area of the slide showed a percentage of positive staining about 50%, the central area of the slide showed significantly weak positive result.
Reproduced with permission from Shi et al., Biotech. Histochem. 2007; 82: 301–309.
Figure 1.1 Comparison of pRB-IHC staining results for frozen and FFPE tissue sections using four AR protocols. All images are arranged in the same order as given in Table 1.3, indicating all scores indicated in the table. T24 and J82 are two cell lines, Ca #1 and Ca #2 are specimens of human bladder cancer, frozen means frozen cells or tissues fixed in acetone, other terms listed in the top line represent FFPE tissue sections after various AR treatments: Low pH, AR solution at low pH value; CAPC, citraconic anhydride solution with boiling; CA98C, citraconic anhydride solution with heating at 98°C; citrate, conventional boiling heating with citrate acid buffer at pH 6.0. Original magnification × 200.
Reproduced with permission from Shi et al., Biotech. Histochem. 2007; 82: 301–309.
See color insert.
Second Step: For further evaluation, a comparative IHC study was performed using citraconic anhydride and conventional AR protocols with a TMA of 31 cases of bladder cancer. Findings are summarized in Table 1.4. Only 27 cases were available for evaluation due to loss of tissue cores for four cases. Among 27 cases, there were 6, 8, and 13 cases for strong, moderate positive, and negative pRB-IHC, respectively. Identical percentages of pRB-positive nuclei were found in all cases, using either of the two protocols for citraconic anhydride or the low pH solution for AR. Inconsistent and significantly weaker nuclear pRB staining results were found when using citrate buffer of pH 6.0 for AR (Table 1.4; Fig. 1.2).
TABLE 1.4 Comparison of pRB-IHC in 27 Cases of FFPE Tissues of Bladder Cancer Using Four Protocols of AR
Notes: CA98°C, heating tissue sections in 0.05% citraconic anhydride at 98°C for 45 min; CAPC, heating tissue sections in 0.05% citraconic anhydride in a plastic pressure cooker using microwave oven for 30 min; Low pH, heating tissue sections in acetic buffer of pH 1–2 for shorter time as described in the text; Citrate, conventional citrate acid buffer 0.01 M at pH 6.0 with same heating condition of a plastic pressure cooker described above.
Reproduced with permission from Shi et al., Biotech. Histochem. 2007; 82: 301–309.
Figure 1.2 Examples of immunostaining intensity from comparison of pRB-IHC in 27 cases of FFPE tissues of bladder cancer (Table 1.4). (A–D) Negative (<10%) showing a few weak positive nuclei (arrows); (E–H) moderate positive (>10%); (I–P) strong positive (>50%). Arrows indicate positive nuclear staining for some lymphocytes or other stromal cells as an internal control. Note the lack of nuclear hematoxylin counterstaining due to low pH AR treatment. The order of cases are indicated in Table 1.4.
Reproduced with permission from Shi et al., Biotech. Histochem. 2007; 82: 301–309.
See color insert.
Third Step: The Western blotting technique, applied to cell extracts, was used to confirm the pRB immunostaining results in two bladder cancer cell lines of T24 and J82, giving quantitative results for pRB in the two cell lines, comparable with that demonstrated by IHC (Fig. 1.3).
Figure 1.3 Western blotting of pRB protein extracted from two fresh cell lines, T24 and J82. The pRB proteins in fresh T24 cell line showed a stronger band than that obtained from J82 cell line. The Western blotting results correlated well with IHC staining intensity (Table 1.3 and Fig. 1.1).
Reproduced with permission from Shi et al., Biotech. Histochem. 2007; 82: 301–309.
Although the novel AR protocol using citraconic anhydride improved the intensity of IHC on FFPE tissue sections for more than half of the antibodies tested, compared to that achieved by other conventional AR protocols, not all antibodies benefitted, which would argue that the citraconic anhydride method does not serve as a truly universal AR pr...
Table of contents
Cover
Half title page
Series page
Title page
Copyright page
PREFACE
CONTRIBUTORS
Part I: RECENT ADVANCES IN ANTIGEN RETRIEVAL TECHNIQUES AND ITS APPLICATION
Part II: STANDARDIZATION OF IMMUNOHISTOCHEMISTRY
Part III: TISSUE/CELL SAMPLE PREPARATION
Part IV: MOLECULAR MECHANISM OF ANTIGEN RETRIEVAL TECHNIQUE
Part V: PROTEOMIC ANALYSIS OF PROTEIN EXTRACTED FROM TISSUE/CELLS
APPENDIX RELATED LABORATORY PROTOCOLS
Index
Color Plates
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Antigen Retrieval Immunohistochemistry Based Research and Diagnostics by Shan-Rong Shi, Clive R. Taylor, Shan-Rong Shi,Clive R. Taylor in PDF and/or ePUB format, as well as other popular books in Biowissenschaften & Biotechnologie. We have over 1.5 million books available in our catalogue for you to explore.