Chronic Obstructive Pulmonary Disease (COPD) is a progressive, largely irreversible lung condition characterised by airflow obstruction. Although cigarette smoking is the single most important risk factor in its development, other associations and risk factors are thought to have increasing relevance throughout the world. COPD is usually managed in primary care, although it is commonly under-diagnosed, and is one of the most common medical conditions necessitating admission to hospital.
The second edition of the ABC of COPD provides the entire multidisciplinary team with a reliable, up-to-date and accessible account of COPD. Extensively updated by experienced clinicians - including new chapters on spirometry, inhalers, oxygen, death, dying and end of life issues - this ABC is an authoritative and practical guide for general practitioners, practice nurses, specialist nurses, medical students, paramedical staff, junior doctors, non-specialist doctors and all other health professionals working in both primary and secondary care.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Division of Applied Health Sciences, University of Aberdeen, Aberdeen, UK and Aberdeen Royal Infirmary, Aberdeen UK
Overview
Chronic obstructive pulmonary disease (COPD) is characterised by largely irreversible airflow obstruction and an abnormal inflammatory response within the lungs
It is the fourth leading cause of death in the United States and Europe
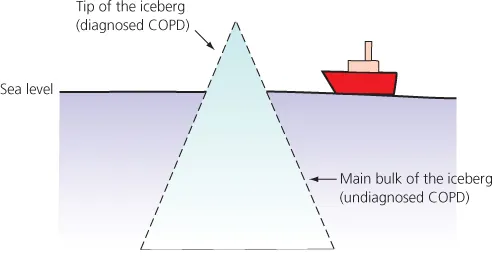
Cases of known COPD are likely to only represent the ‘tip of the iceberg’ with as many individuals undiagnosed
Other conditions also cause progressive airflow obstruction and these need to be differentiated from COPD
COPD is usually caused by cigarette smoking, but pipe, cigar and passive smoking, indoor and outdoor air pollution, occupational exposures, previous tuberculosis and repeated early life respiratory tract infections have all been implicated in its development
The prevalence of COPD in never smokers (estimated to be between 25 and 45% worldwide) is higher than previously thought; the use of biomass fuel (mainly in developing countries) is one of the main risk factors
Definition
Chronic obstructive pulmonary disease (COPD) is a progressive disease characterised by airflow obstruction and destruction of lung parenchyma. The current definition as suggested by the American Thoracic and European Respiratory Societies is as follows:
COPD is a preventable and treatable disease state characterised by airflow limitation that is not fully reversible. The airflow limitation is usually progressive and associated with an abnormal inflammatory response of the lungs to noxious particles or gases, primarily caused by cigarette smoking. Although COPD affects the lungs, it also produces significant systemic consequences.
COPD is the preferred term for the airflow obstruction associated with the diseases of chronic bronchitis and emphysema (Box 1.1). A number of other conditions are associated with poorly reversible airflow obstruction—for example, cystic fibrosis, bronchiectasis and obliterative bronchiolitis. These conditions need to be considered in the differential diagnosis of obstructive airway disease, but are not conventionally covered by the definition of COPD. Although asthma is defined by variable airflow obstruction, there is evidence that the airway remodelling processes associated with asthma can result in irreversible progressive airflow obstruction that fulfils the definition for COPD. Because of the high prevalence of asthma and COPD, these conditions co-exist in a sizeable proportion of individuals resulting in diagnostic uncertainty.
Box 1.1 Definitions of conditions associated with airflow obstruction
COPD is characterised by airflow obstruction. The airflow obstruction is usually progressive, not reversible and does not change markedly over several months. The disease is predominantly caused by smoking.
Chronic bronchitis is defined as the presence of chronic productive cough on most days for 3 months, in each of 2 consecutive years, in a patient in whom other causes of productive cough have been excluded.
Emphysema is defined as abnormal, permanent enlargement of the distal airspaces, distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis.
Asthma is characterised by reversible, widespread and intermittent narrowing of the airways.
Epidemiology
Prevalence
The prevalence of COPD varies considerably between epidemiological surveys. While this reflects the variation in the prevalence of COPD between and within different countries, differences in methodology, diagnostic criteria and analytical techniques undoubtedly contribute to disparities between studies.
The lowest estimates of prevalence are usually based on self-reported or doctor-confirmed COPD. These estimates are usually 40–50% of the prevalence rates derived from spirometric indices. This is because COPD is underdiagnosed due to failure to recognise the significance of symptoms and relatively late presentation of disease (Figure 1.1). Estimates of the prevalence of spirometric-defined COPD using UK criteria are less than the estimates based on European and US criteria (Chapter 4).
Figure 1.1 Known cases of COPD may represent only the ‘tip of the iceberg’ with many cases currently undiagnosed.
In the United Kingdom, a national study reported that 10% of males and 11% of females aged 16–65 years had an abnormally low forced expiratory volume in 1 second (FEV1). Similarly, in Manchester, non-reversible airflow obstruction was present in 11% of subjects aged >45 years, of whom 65% had not been diagnosed with COPD. In Salzburg, Austria, doctor-confirmed COPD was reported by 5.6% of adults aged ≥40 years in a population survey; however, on evaluation using spirometric indices, 10.7% fulfilled UK criteria and 26.1% fulfilled European/US criteria. In the United States, the reported prevalence of airflow obstruction with an FEV1 < 80% predicted was 6.8%, with 1.5% of the population having an FEV1 < 50% and 0.5% of the population having more severe airflow obstruction (FEV1 < 35% predicted). As in the United Kingdom, around 60% of subjects with airflow obstruction had not been formally diagnosed with COPD.
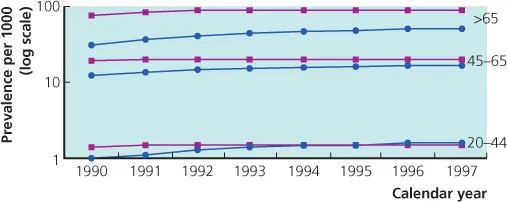
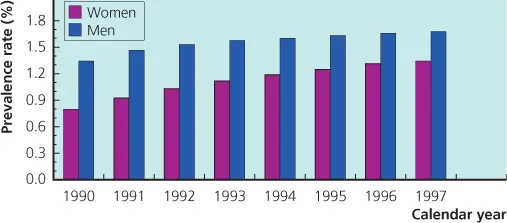
In England and Wales, it has been estimated that there are about 900,000 patients with diagnosed COPD. However, after allowing for underdiagnosis, the true number of individuals is likely to be about 1.5 million, although a figure as high as 3.7 million has been suggested. The mean age of diagnosis in the United Kingdom is around 67 years, and the prevalence of COPD increases with age (Figure 1.2). It is also more common in males and is associated with socio-economic deprivation. In the United Kingdom, the prevalence of COPD in females is increasing (Figures 1.3 and 1.4). For example, it was considered to be 0.8% in 1990 and had risen to 1.4% in 1997. In males, the prevalence appears to have plateaued since the mid-1990s. Similar trends have been reported in the United States. These time trends in prevalence probably reflect the gender differences in cigarette smoking since the 1970s.
Figure 1.2 Prevalence (per 1000) of diagnosed COPD in UK men (
) and women (
) grouped by age, between 1990 and 1997. (Reproduced with permission from Soriano JB, Maier WC, Egger P, et al. Thorax 2000; 55: 789–794)
Figure 1.3 Prevalence of diagnosed COPD in UK men and women (per 1000) between 1990 and 1997. (Reproduced with permission from Soriano JB, Maier WC, Egger P, et al. Thorax 2000; 55: 789–794)
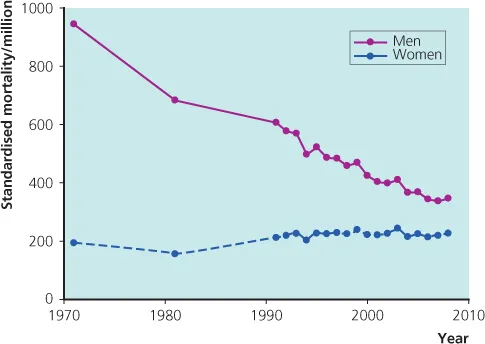
Figure 1.4 UK death rates from COPD since 1971. Age-standardised mortality rates per million: based on the European Standard Population. Figure derived with data from Death registrations, selected data tables, England and Wales 2008. Office for National Statistics, London. http://www.statistics.gov.uk/downloads/theme_health/DR2008/DR_08.pdf. (Accessed 12/09).
Mortality
COPD is the fourth leading cause of death in the United States and Europe. Globally, COPD was ranked the sixth most common cause of death in 1990; however, with increases in life expectancy and cigarette smoking, particularly in developing countries, it is expected that COPD will be the third leading cause of death worldwide by 2020. In the United Kingdom in 2008, there were approximately 25,000 deaths due to COPD; 13,000 of these deaths were in males and 12,000 in females. These figures suggest that COPD underlies 4.9% of all deaths (5.4% of male deaths and 4.4% of female deaths) in the United Kingdom.
In the United Kingdom, over the last 30 years, mortality rates due to COPD have fallen in males and risen in females. However, it seems likely that in the near future, there will be no gender difference. In the United States, the most recent data between 2000 and 2005 suggest that 5% of deaths are a consequence of COPD. Although overall, the age-standardised mortality rate was stable at about 64 deaths per 100,000, the death rate in males fell from 83.8/100,000 in 2000 to 77.3/100,000 in 2005 and increased in females from 54.4/100,000 to 56.0/100,000.
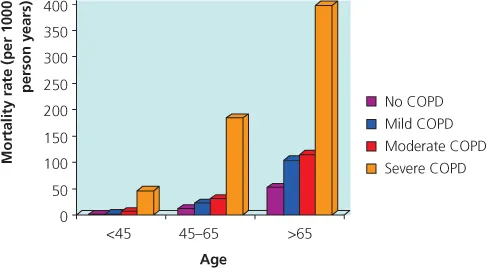
Mortality rates increase with age, disease severity and socio-economic disadvantage (Figure 1.5). On average, in the United Kingdom, COPD reduces life expectancy by 1.8 years (76.5 vs 78.3 years for controls); mild disease reduces life expectancy by 1.1 years, moderate disease by 1.7 years and severe disease by 1.4 years.
Figure 1.5 UK deaths from COPD (per 1000 person years) by age and severity of COPD. Figure derived with data from Soriano JB, Maier WC, Egger P, et al. Recent trends in physician diagnosed COPD in women and men in the UK. Thorax 2000; 55: 789–794.
Morbidity and Economic Impact
The morbidity and economic costs associated with COPD are very high, generally unrecognised and more than twice that associated with asthma. The impact on quality of life is particularly high in patients with frequent exacerbations, although even those with mild disease have an impaired quality of life.
In the United Kingdom, emergency hospital admissions for COPD have steadily increased as a percentage of all admissions from 0.5% in 1991 to 1% in 2000. In 2002/2003, there were 110,000 hospital admissions for an exacerbation of COPD in England with an average duration of stay of 11 days, accounting for 1.1 million bed days. At least 10% of emergency admissions to hospital are as a consequence of COPD and this ...
Table of contents
Cover
Title Page
Copyright
Contributors
Foreword
Chapter 1: Definition, Epidemiology and Risk Factors
Chapter 8: Pharmacological Management (II) – Oral Treatment
Chapter 9: Inhalers
Chapter 10: Oxygen
Chapter 11: Exacerbations
Chapter 12: Non-invasive Ventilation
Chapter 13: Primary Care
Chapter 14: Death, Dying and End-of-Life Issues
Chapter 15: Future Treatments
Index
Advertisement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access ABC of COPD by Graeme P. Currie in PDF and/or ePUB format, as well as other popular books in Medicine & Pulmonary & Thoracic Medicine. We have over 1.5 million books available in our catalogue for you to explore.