Speech and Song at the Margins of Global Health tells the story of a unique Zulu gospel choir comprised of people living with HIV in South Africa, and how they maintained healthy, productive lives amid globalized inequality, international aid, and the stigma that often comes with having HIV. By singing, joking, and narrating about HIV in Zulu, the performers in the choir were able to engage with international audiences, connect with global health professionals, and also maintain traditional familial respect through the prism of performance. The focus on gospel singing in the narrative provides a holistic viewpoint on life with HIV in the later years of the pandemic, and the author's musical engagement led to fieldwork in participants' homes and communities, including the larger stigmatized community of infected individuals. This viewpoint suggests overlooked ways that aid recipients contribute to global health in support, counseling, and activism, as the performers set up instruments, waited around in hotel lobbies, and struck up conversations with passersby and audience members. The story of the choir reveals the complexity and inequities of global health interventions, but also the positive impact of those interventions in the crafting of community.
eBook - ePub
Speech and Song at the Margins of Global Health
Zulu Tradition, HIV Stigma, and AIDS Activism in South Africa
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Speech and Song at the Margins of Global Health
Zulu Tradition, HIV Stigma, and AIDS Activism in South Africa
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Publisher
Rutgers University PressYear
2019Print ISBN
9780813597713
9780813597720
eBook ISBN
9780813597737
1 • INTRODUCTION
It is already dark when we arrive at the funeral. The event is being held at the rural farm of two sisters, Zethu and Amahle, who are members of a unique Zulu gospel choir.1 The funeral is for their brother. The drive from Durban, a cosmopolitan metropolis and port on the Indian Ocean, to the South African countryside took several hours. So far, what I know of this rural area includes a two-lane road mauled by corporate timber and sugarcane trucks, a tiny town whose main draw is a livestock auction, the dirt wheel-ruts I nervously negotiate in my tiny, two-wheel-drive rental car, and the sound of cows mooing nearby. When I park by a goat shed, five isiZulu-speaking2 South Africans—members of a gospel choir with whom I have begun to conduct fieldwork—extract themselves from the small car.
On the way to the funeral, a choir member named Fanele had begun to ask me questions about my research. What were my goals? How did I plan to contribute to the activities of the choir? Was I interested in music? Language? HIV/AIDS? She listened carefully to my responses. Then she told me that people living with HIV were tired of researchers who came, asked their questions, and then left. Sometimes, Fanele explained, infected individuals just told researchers what they thought the researchers wanted to hear, took payment, and waited for the researchers to go. If I wanted to know more about what was going on, I would have to stick around.
After we arrive at the farm, I am asked if I want to participate in the evening’s events. I nervously reply, “yes,” and I am led to the family’s roundhouse. The roundhouse is a family ritual center, a large, round, single-room structure with a small Christian altar. Bull horns hang on the wall, and a central post shoots upward to support a conical metal roof. The roundhouse is a space to commune with one’s ancestors during family events, such as deaths, births, and birthdays. It had once been the one-room home of the family before a larger, rectangular house with bedrooms, a living room, and a kitchen had been built. Days before the funeral, the body and soul of the deceased had been carefully led by a spiritual leader, Baba Shangane, to the roundhouse from a township near Durban.
From outside, I can hear a number of people singing Zulu hymns. I have no idea what to expect. I have never been to a Zulu funeral before. I take a deep breath and walk into the room. It is like jumping into cold water. I feel out of place. Fifty pairs of eyes look up at me.
The father of the deceased, who I would later learn to call Baba (father), quickly pulls up a plastic chair and kindly asks me to sit next to him. The hymns continue. Baba is a black South African man who lived through both the official beginning of apartheid in 1948 and its legislative dismantling in 1994. He labored in the manufacturing industry and worked with his brothers to maintain the family farm where I now sit. He also saved up to buy and maintain a four-room, government-built, cinder-block home in a formerly black township near Durban, where Amahle and Zethu now live with their sister, their nephew, and Zethu’s son. In the early 2000s, at a time when some parents disowned children who disclosed their HIV-positive status, Baba had responded with compassion and love upon hearing the news that two of his daughters were HIV positive. Though I did not learn this until later on, his son, whom he is burying at this funeral, died as a result of HIV infection.
In the familial roundhouse, knee-to-knee and shoulder-to-shoulder with Baba, I glance around the room. I notice that all the men who are present sit on chairs or benches, whereas the women sit on mats on the floor. These observations are interrupted by a question:
“Why are you not singing?” Baba asks in English. “Are you not Christian?”
“I don’t know these songs in Zulu,” I respond, answering the first question and evading the next. My answer seems to satisfy him. With each song, funeral-goers seamlessly weave their voices together in four-part harmony. When one hymn ends, someone in the group takes the initiative and begins the next song. The effect is almost hypnotic. Minutes and hours disappear over a temporal horizon, replaced by the rhythmic cycles of song into which participants immerse themselves. After a number of songs have begun and ended, Amahle asks me if I would like to go and sleep. She leads me to her father’s bed. She explains that neither he nor the others would sleep that night, but that it would be inappropriate for me to be present for some of the night’s events. So, I sleep.
In the morning after I awaken, I sit quietly in a small living room watching Amahle, Zethu, and other women prepare breakfast. Two couches create a border around a cowhide rug that lies over a polished concrete floor. In the corner, a small black-and-white TV is attached to what appears to be a car battery. There is no electricity in the house, no toilet, and no municipal water, but a gas stove (fueled by paraffin) and a large water tank ensure that the kitchen is a comfortable space in which to cook. I look out a window and see some men on the edge of a cornfield, taking turns using a pickax and shovel to dig a grave.
Soon, one man comes to find me in the house. He invites me to come with him, instructing me, “No Steve—you mustn’t sit with the women here. Come and sit with the men outside.” I go with him. I try to interact with the other men, even though at this early point in my fieldwork I am not a fluent isiZulu speaker. However, many of the men speak English. At one point, someone sits down with me and asks where I am from.
“Oh, you’re American,” he muses. “Where is your camera? Don’t you have a camera?”
“No,” I reply. “Well, I do have a camera, but I wasn’t sure about using it. I just wasn’t sure if it was appropriate or not, and I was even afraid to ask because I thought it would be disrespectful.”
He zeroes in on the word “disrespectful,” quickly responding, “Ah, that’s good. That shows that you already know something about Zulu culture.”
Later, as I stand talking with that man and a few older men, he exclaims, “You see, Steve is here with his heart. He didn’t come with his video camera to shoot pictures and then take them back to America. He came here with his heart to experience our culture.” This statement about coming first and foremost as a person to experience and understand the lives of others would stay with me throughout my research.
The daytime funeral service is held inside a large, white vinyl tent pitched next to the house. Amid the ethos of “living positively” maintained by the Thembeka choir, the funeral is a reminder of the constant stream of tragedies in a nation where as much as 20 percent of the population may be infected with HIV. Rows of white plastic chairs face an open casket, in front of which a number of pastors and religious leaders from various groups take turns sermonizing. At this funeral, unlike many American funerals, any religious leader who wishes to speak is free to do so. From the rear of the tent, I watch and listen as the coffin is shut and Amahle, sister of the deceased, calls out in lament.
After he died, Amahle and Zethu found a shoebox full of unopened antiretroviral medication (ARV) under their brother’s bed. He had been going to collect the medication but not taking it. Presumably the act of going to the clinic was meant to satisfy his activist sisters that he was receiving treatment. The tragedy of his passing was compounded by the knowledge that the death might have been prevented. In one family, in one home, three siblings were living with HIV. Why did one sibling reject medical treatment while the other two thrived?
OVERVIEW
I traveled to Durban, South Africa, in early February 2008, to stay for a period of nine months, conducting ethnographic fieldwork on language, music, culture, and HIV/AIDS. Upon arrival, I hoped to focus my research on a choir consisting of people living with HIV. The choir, called the Thembeka choir, was part support group, part activist organization, and part performance troupe. The choir had been on tour five times to the United States and once to England, the trips paid for by an international Christian aid group and donations. The choir could be labeled a biosocial group—that is, a group in which membership is in part dependent on a shared biomedically defined characteristic (in this case, diagnosis with HIV infection) (Rabinow 1992). Combining this concept of the biosocial group with linguistic anthropology’s notion of the speech community, in this book I describe the choir as a bio-speech community to help model how the choir community intersected with other groups (e.g., biomedical research organizations, activist groups, Christian aid groups) that shared biomedical orientations toward HIV/AIDS (see Bucholtz 1999; Eckert and McConnell-Ginet 1998 for critiques of the speech community concept; more to come on this). When I began fieldwork, I was interested in the choir because it was an instance of an intervention that seems to be succeeding amid the many disappointments of the South African epidemic. I was hoping to complete what Joel Robbins (2013) later theorized as “an anthropology of the good”; though as fieldwork progressed I learned that the choir’s situation was more ambivalent and complex than I had initially imagined. I was also interested in the choir because this successful intervention involved music. I arrived in Durban with twenty-three years of musical training, including fifteen years of work as a jazz saxophone player and an undergraduate degree in ethnomusicology. Like other researchers before me (e.g., Barz 2006; McNeill 2011), I planned to use music as an ethnographic research tool in settings around HIV/AIDS. Prior to my arrival, I had also studied anthropology (earning a B.A. and an M.A. in the field), specializing in the subfields of linguistic and medical anthropology. One of my research goals was to understand how members of the Thembeka choir used language and music to construct support and engage in HIV activism amid the intense stigma that characterized the South African AIDS epidemic. Nine months of fieldwork also resulted in learning about research participants’ translinguistic practices—that is, how they incorporated multiple linguistic codes into a hybrid communicative toolkit (García 2009; Reynolds and Orellana 2015)—to transpose biomedical models of HIV across the borders of multiple communities at the margins of global health (more to come on this).
This book synthesizes theoretical lenses from linguistic, medical, and psychological anthropology to advance a new perspective on the activities, roles, and positioning of marginalized aid recipients in global health. This perspective emerged out of my encounters with members of the Thembeka choir. When I traveled to Durban, South Africa, in 2008 to study communication, culture, and HIV/AIDS stigma, I expected to hear stories of death, despair, exclusion, and suffering; such stories were indeed prominent. However, the choir promoted a different outlook—one rooted in play and creativity. At choir rehearsals and social gatherings, group members sang songs together about HIV and Christian faith. They also told stories and joked with one another about HIV. Vocal play was interconnected with play (in the nominal sense of the word) in the choir’s structural positioning at the borders of both global health and Durban-area communities. Located at the margins of several networks, the Thembeka choir was paradoxically at the center of multiple overlapping speech communities associated with global health in Durban. While members of these communities (including the choir community) came from numerous distinct ethnic, racial, class, educational, and national backgrounds, one thing that provided a place of contact and overlap was a set of biomedical perspectives toward HIV/AIDS. Linking anthropological scholarship on biosociality and biopower with research on speech communities and biocommunicability, I coin the term “bio-speech communities” to emphasize research participants’ shared orientations toward powerful biomedical perspectives on HIV/AIDS.
Through performance in speech and song, specifically by transposing AIDS across social and cultural contexts, choir members worked to create the social and economic space not only to exist but also to thrive at the margins of global health at a time when many other infected individuals were depressed or dying. Here, I adapt the term “transposition” from musical terminology (cf. Jakobson 1959: 238; Silverstein 2003). I use the term as a way to link research in medical and psychological anthropology on explanatory models/medical pluralism and the “translation” of scientific objects with scholarship in linguistic anthropology on code-switching/translanguaging. Generally, to transpose means to move an entity from one context or setting to another. In music, specifically, to transpose means to shift a song from one harmonic center (or key) to another. While each transposed performance includes the same melody and harmony, the shift in harmonic center may give the same song a different feel (e.g., as one moves from the bass tones of one harmonic center to the treble tones of another, or vice versa). In jazz music, performers sometimes improvise or plan such transpositions in the midst of a song as a way to shift the feel of the performance. Analogously, while the core meaning of biomedical terminology remained the same when Thembeka choir members used biomedical terminology in distinct linguistic (English and isiZulu) and community contexts (in choir rehearsals, at a research clinic, in encounters with other support group members), a shift in the indexical and semantic significance of words sometimes occurred.
While this book analyzes the language of HIV support and activism in South Africa, the lessons learned from the analysis may be applicable to many global health contexts, and to examinations of marginality and international aid more broadly. Drawing from research on globalization and science–technology–society studies, anthropologists emphasize that global health comprises complex networks of circulating discourses, money, technologies, medicine, people, and pathogens (Biehl and Petryna 2013; Brada 2017; Fassin 2012; Nguyen 2010). Within and among networks, the circulation of these resources, discourses, people, and pathogens is uneven. The linguistic anthropological theorizations of play and performance that are utilized in this book place the actions of marginalized persons at the center of the analysis, demonstrating how such persons engage with, and in some cases transform, the overlapping community-wide, national, and transnational institutional and societal structures that have marginalized them.
This ethnography is based on fieldwork conducted in Durban, South Africa. With over two million inhabitants in the greater metropolitan area, Durban is the largest city in the province of KwaZulu-Natal (figure 1.1). The city is home to the second-busiest port in Africa (after Port Said, Egypt) and is the epicenter of the South African AIDS epidemic. In 2008, by some estimates, as much as 35 percent of adult residents of reproductive age in the province were HIV positive, and 10.6 percent of South Africans were HIV positive (Shisana et al. 2009). In other words, Durban is deeply enmeshed in patterns of inter- and intranational circulation associated with global capitalism, global health, and the AIDS pandemic. About the pandemic, a Joint United Nations Programme on HIV/AIDS (UNAIDS) report indicates that in the mid-2000s AIDS was the worldwide leading cause of death among persons aged 15–19 and remained the leading cause of death in Africa through 2010 (cited in Bulled 2015: 20). The International AIDS Conference has been held twice in Durban, first in 2000 and then in 2016. By 2012, the national estimate for HIV prevalence had gone up to 12.2 percent, and KwaZulu-Natal remained the state with the most infections (Shisana et al. 2014). These statistics and the conference’s location are an indication that Durban has been not only an epicenter of the pandemic but also a central location for global health researchers, scholars, doctors, and media professionals interested in HIV/AIDS.
As in other global health contexts, Durban global health in 2008 included a dizzying array of interests, institutions, and actors, including the South African National Department of Health, government-run and private hospitals, South African nonprofit organizations (including activist organizations such as LoveLife and the Treatment Action Campaign [TAC]), international nonprofit organizations, the World Health Organization (WHO), UNAIDS, The Bill and Melinda Gates Foundation, and the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR). For people living with HIV, many of these groups provided potential access to money, medication, and treatment. Many members of the Thembeka choir were active in multiple HIV/AIDS organizations focused on prevention, treatment, and activism, and the choir itself was an outgrowth of these organizations and efforts. These governmental and nongovernmental institutions also provided communicative and ideological links to global health that were significant as an alternative to the HIV stigma that many infected individuals experienced in their home and work life.
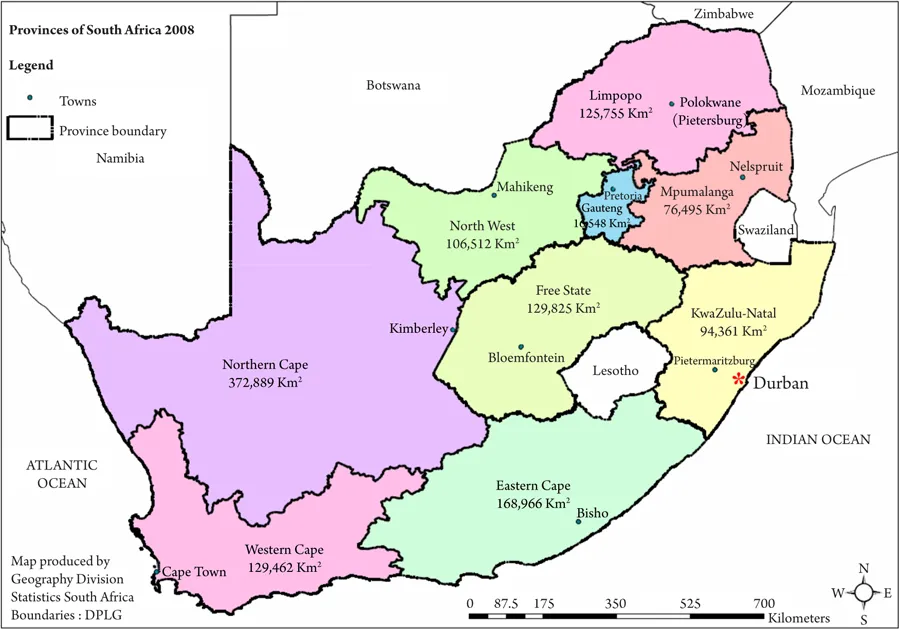
FIGURE 1.1. Provinces of South Africa, modified by Steven P. Black, original from Statistics South Africa 2008. All images by Steven P. Black unless otherwise noted.
Researcher Positionality
This research project presented a number of challenges and opportunities with respect to my positioning among research participants, public health researchers, and scholars. First, in conducting this research I have struggled with the question of research participant anonymity with regard to the publications and artistic products of other researchers. In my research, I use pseudonyms to refer to people and organizations. This was both stipulated in institutional review board (IRB) documents and agreed upon in consultation with choir members. At the outset of my fieldwork in 2008, it seemed to me that anonymity needed to be maintained amid the intense stigmatization of HIV in South Africa. My decision to use pseudonyms contrasts with the American documentary filmmakers and with another scholar who conducted research with the choir prior to my arrival. These scholars use choir members’ real names in publications. This puts me in the awkward position of being ...
Table of contents
- Cover
- Title Page
- Copyright
- Dedication
- Contents
- List of Figures
- Transcription Conventions, Orthography, and Morpheme Labels
- 1. Introduction
- 2. Conducting Ethnographic Fieldwork amid Globalized Inequities and Stigma
- 3. The Embodied Reflexivity of a Bio-Speech Community
- 4. The Power of Global Health Audiences
- 5. HIV Transposition amid the Multiple Explanatory Models of Science, Faith, and Tradition
- 6. The Linguistic Anthropology of Stigma
- 7. Performance and the Transposition of a Global Health Ethics of Disclosure
- 8. Conclusion
- Acknowledgments
- Notes
- References
- Index
- About the Author
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Speech and Song at the Margins of Global Health by Steven P. Black in PDF and/or ePUB format, as well as other popular books in Social Sciences & AIDS & HIV. We have over 1.5 million books available in our catalogue for you to explore.