Cracking the Code covers the basics of the contents of patients' medical notes. Common medical terminology used in reviewing physiological systems is briefly explained. Commonly encountered investigative procedures are defined and their use explained. Medical laboratory tests are similarly explored.Much of this book concentrates on the secondary care environment because this remains the main setting in which healthcare professionals have free and open access to patient medical notes. However, the expanding roles of healthcare professionals in the primary care sector mean that all practitioners need to be able to 'unlock the code' of medical terminology and abbreviations. It is hoped that this book will therefore be of use not only to the undergraduate pharmacy students for whom it was originally developed, but also to other healthcare professionals who routinely access patient medical notes.This new edition has been revised and updated to incorporate measurements of body weight and surface area, capillary blood gases, sepsis screening, common drug serum levels, and changes to the reporting of cardiac troponins.
eBook - ePub
Cracking the Code: A quick reference guide to interpreting patient medical notes
2nd Edition
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Cracking the Code: A quick reference guide to interpreting patient medical notes
2nd Edition
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSection 1
Medical terminology
In order to interpret a patient’s medical notes accurately and with confidence, it is essential to have a good grasp of medical terminology. Some of the terms that are commonly encountered may appear to be very long and complicated but they are generally built up from smaller ‘building blocks’. Once the longer terms have been broken down into their constituent blocks, the meaning becomes much clearer.
Medical terms have three basic components: the root, which forms the basis of the word; a prefix – any syllables added in front of the root to modify it and a suffix – any syllables added after the root to modify it. Knowledge of the meanings of a few common roots, prefixes and suffixes enables the understanding of the majority of commonly encountered medical terms.
For example:
| (PSEUDO) | (HYPO ) | (PARA) | (THYROID) | (ISM) |
| (false) | (under) | (beside) | (thyroid) | (condition) |
i.e. a condition resembling underactivity of the parathyroid glands.
Tables 1.1 and 1.2, on page 2, contain some of the common roots, prefixes and suffixes that are encountered in clinical practice.
Table 1.1: Common medical prefixes, suffixes and roots
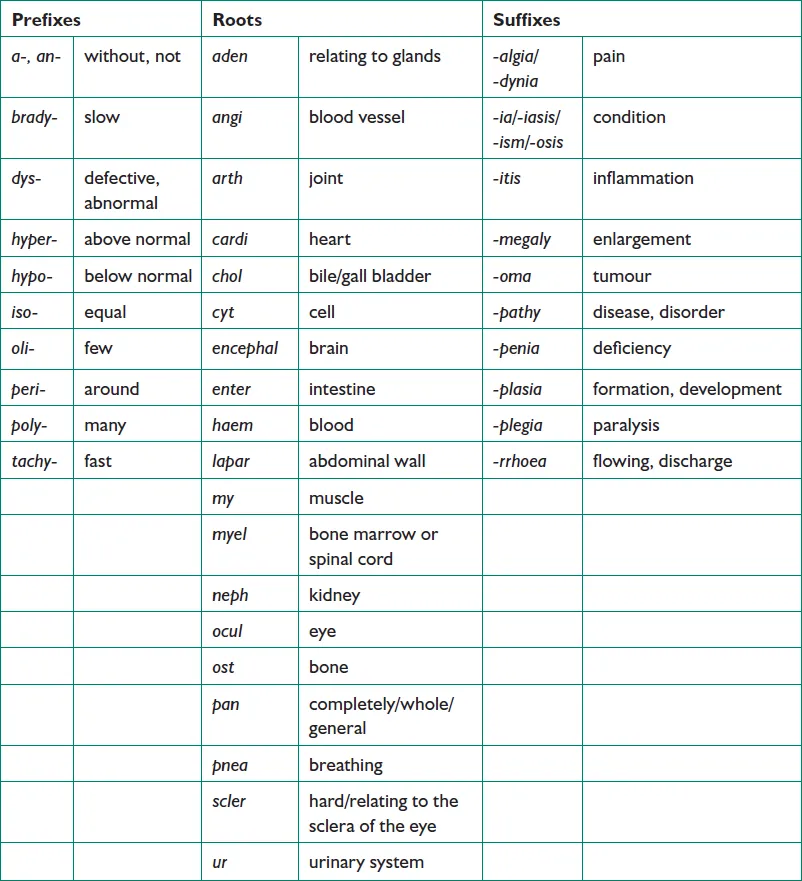
Table 1.2: Common surgical suffixes
| -centesis | surgical puncture (used for aspiration) |
| -desis | binding |
| -ectomy | excision or removal of a body part |
| -plasty | repair, reconstruction |
| -rrhapy | surgical suturing |
| -scopy | use of a viewing instrument |
| -stomy | creation of an opening |
| -tomy | the act of cutting, making an incision |
Section 2
Patient medical notes
To be involved effectively in the clinical decision-making process, it is important to be able to understand and utilise the information to be found in the patient medical notes. On occasions it is also necessary for the pharmacist to record their interventions in a patient’s medical notes.
The medical notes are a chronological record of all significant aspects, including drug treatment, of a patient’s care. These are completed for both inpatient stays and for outpatient clinic visits. As a clinical pharmacist you will frequently intervene directly in the care of patients to ensure the safety and efficacy of their treatment. If you do need to intervene in a patient’s drug treatment, there are a number of ways in which you can convey this information to the prescriber(s) concerned.
Face to face with the prescriber
This is much the best way to deal with any concerns you have. The modifications you wish to recommend to the prescriber can be discussed and you will all have the information you require to hand. The prescriber is unlikely to document your intervention in the patient’s medical notes.
Bleeping or phoning the doctor
If the prescriber is not available for a face to face discussion and the intervention you wish to make is urgent, this is the method used for contacting the prescriber. However, it may not be a convenient time for the prescriber to talk to you. Again, it is unlikely that the prescriber will document your intervention in the patient’s medical notes.
Leaving a note on the prescription
This is often used as a method of communication in the hospital environment, particularly if the prescriber is a surgeon, is in theatre and cannot be disturbed. However, such notes are easily lost and if your intervention is not addressed by the prescriber it is difficult to say whether the prescriber saw your note and chose to ignore it, or whether your note was seen at all. Again there is no permanent record of your intervention.
Leaving a message with another member of staff
Your message may not be passed on correctly, if at all. Again there is no permanent record of your intervention.
The following are examples of when you, as a clinical pharmacist, should document your interventions in a patient’s medical notes:
•When you recommend that a drug is initiated or discontinued
•When you have discovered that an adverse drug reaction has occurred
•When you discover that the patient is not, or has not been, compliant with their medication
•When your input has been requested by the medical team
•When a critical change to a dosage regimen has occurred
•When an important recommendation has not been followed
•When your written communication would facilitate a review of the patient’s drug treatment.
General Layout
The way in which patient medical notes are arranged varies from Trust to Trust. However, the following sections are usually present; it is the order in which they are presented that differs.
Inpatient admissions
The current admission may be found to the front or to the back of this section. All admission notes will contain the same information and previous admissions may be useful for obtaining certain information such as previous drug history (which may not be accurate!).
The current admission usually contains the following information: case history, systems enquiry and examination, differential diagnoses/provisional diagnosis, investigations, drug history, progress.
Outpatient notes
These are often less precise than a full admission, usually consisting of the specific problem, progress since last visit, any relevant measurements and test results, and drug therapy.
Investigations
This section contains, if printed, the clinical chemistry, haematology and microbiology reports, along with the results of X-rays, scans, biopsies, etc. Investigations may not always be recorded in the notes, but available electronically elsewhere.
Letters
Discharge, clinic and referral (from GPs and other consultants) letters will be included.
Other information
This will include copies of previous discharge prescriptions, drug treatment sheets, and nursing notes.
Breakdown of Medical Notes
Case history
The case history is the information obtained from the patient on admission. The process is known as ‘clerking’ and is usually performed by the on-call doctor (either the Foundation Year 1 (FY1) doctor or the Foundation Year 2 (FY2) doctor) or in some places in pre-admission clinics. A patient may be admitted to hospital via several routes, the most common being: elective (i.e. a planned, booked admission), acute via Accident and Emergency, acute via GP referral or acute self-referral.
Presenting complaint (PC)
These are the main symptoms that have led to the referral and admission to hospital. The PC may also be referred to as ‘CC’ (chief complaint) or ‘C/O’ (complains of).
History of presenting complaint (HPC)
This consists of the symptoms experienced in the recent past leading up to the referral, usually with reference to the presenting complaint, as...
Table of contents
- Cover Page
- Title Page
- Copyright
- Contents
- About the contributors
- Introduction
- Section 1: Medical terminology
- Section 2: Patient medical notes
- Section 3: Investigative procedures
- Section 4: Laboratory reports
- Section 5: Medical abbreviations
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Cracking the Code: A quick reference guide to interpreting patient medical notes by Katie Maddock in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.