![]()
Women’s health
Menorrhagia
• Heavy periods, often defined as blood loss >80 mls.
• Cause is often not known, and this is referred to as ‘dysfunctional uterine bleeding’.
• Other causes include fibroids, endometriosis, IUD in situ or hypothyroidism.
• Management includes LNG-IUS, tranexamic acid, COCP or surgical options.
Data gathering
Open question
• “Can you tell me more about the heavy periods that you’ve been experiencing?”
Focused/closed questions
| |
HPC: | “When did the heavy periods first start?”
“Was the heavy bleeding sudden in onset?” (red flag)
“How many times do you change pads/tampons in a typical day?”
“Do you get any clots in the blood or any flooding?”
“Are your periods more painful than usual?”
“Do you get any abdominal pain or abdominal bloating?”
“Are your periods regular? When was your last menstrual period?”
“Do you get any bleeding in between your periods or after sex?” (red flag)
“Are you using any contraception at present? If so, what?”
“When was your last smear test?”
“Any abnormal discharge or risks of any sexually transmitted infections?” |
PMH: | Any other medical conditions? Any previous gynaecological surgery? Any previous pregnancies? |
DH: | “Are you on any regular medications?” (specifically enquire about aspirin and anticoagulants) |
FH: | Any conditions that run in the family? Any bleeding disorders? |
ICE: | “Do you have any thoughts as to what might be causing the heavy bleeding?”
“How is this problem affecting your day to day life?” |
Examination: | • Abdominal/pelvic examination (red flags include pelvic mass and features of PID). • Speculum examination. N.B. Offer chaperone. |
Clinical management
Investigations
• Blood tests – FBC, TFTs (only if symptomatic).
• Vaginal/endocervical swabs for MC&S and STI screen (if at risk).
• Ultrasound scan of pelvis (if concerned about structural abnormality).
Explanation to patient
• Heavy periods often occur because the amount of a chemical called prostaglandin is increased in the lining of the womb.
• It can also be caused by fibroids (benign growths in the womb), endometriosis (endometrial tissue grows outside the womb) or a hormonal problem.
Management
• Menstrual diary.
• LNG-IUS (Mirena) – reduces heavy menstrual bleeding (NICE first line).
• Medications – tranexamic acid, COCP, norethisterone.
• Safety net – to see GP if problem not improving.
• Surgery – endometrial ablation, hysterectomy.
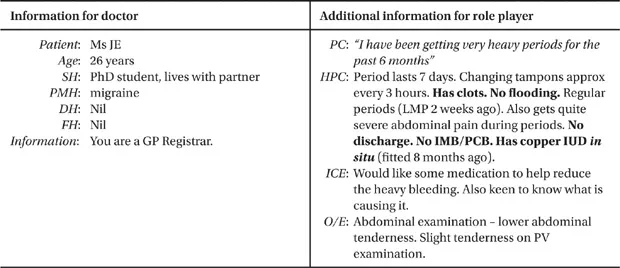
Role play
Amenorrhoea
• Absence or cessation of menses, either classified as primary amenorrhoea (menses not occurring by the time of expected menarche) or secondary amenorrhoea (absence of menstruation for at least 6 consecutive months in women with previously normal and regular menses).
• Causes of primary amenorrhoea include constitutional delay, genito-urinary malformation, Turner syndrome and testicular feminisation.
• Causes of secondary amenorrhoea include hypothalamic failure, pregnancy and lactation, premature ovarian failure, weight loss, polycystic ovarian syndrome and depot or implant contraception.
Data gathering
Open question
• “Can you tell me more about the problem with your periods?”
Focused/closed questions
| |
HPC: | “Have you ever had periods? If so, when was your last menstrual period?”
“At what age did you start having periods (if secondary amenorrhoea)?”
“Is there any chance you could be pregnant?”
“Are you sexually active at present?”
“Have there been any recent change in your weight or any increase in exercise?”
“Have you been more stressed than usual recently?”
“Have you noticed any changes to your skin or hair?”
“Any lower abdominal pain?” (haematocolpos)
“Any hot flushes or vaginal dryness?” (menopause/premature ovarian failure)
“Have you ever had problems trying to get pregnant?”
“Any headache, problems with your vision or leakage of milk from your breasts?” (red flags) |
PMH: | Any medical conditions? PCOS? Thyroid problems? Depression? Eating disorders? Previous surgery? |
DH: | “Do you take any regular medications?” Any hormonal contraceptives? Antipsychotics? Previous radiotherapy or chemotherapy? Steroids? |
FH: | Any family history of menstrual problems? “When did your mother and sister(s) start their periods?” Any family history of stopping periods before 40 years of age? |
SH: | Occupation/Studying? Stress? Who lives with you at home? Any problems? Illicit drug use, e.g. cocaine or opiates? |
ICE: | “Do you have any thoughts as to why your periods might have stopped?” |
Examination
(based on NHS CKS, 2009, Amenorrhoea – management):
| |
| • BMI, BP. • Examine for secondary sexual characteristics, e.g. Tanner Stages (N.B. no intimate examinations in the CSA). • Examine for hirsutism, clitoromegaly, galactorrhoea and haematocolpos (if appropriate from history). • Thyro... |