Endodontic retreatment is technically more difficult to perform, involves greater risks, and is more unpredictable clinically compared with primary endodontic treatment. This book addresses topics such as indications for endodontic retreatment; safe and efficient removal of existing restorations and obturation material; challenges such as fractured instruments, hard pastes, blockages, and negotiation of the canal; treatment of perforations; management of a tooth with a wide-open apex; and assessment of prognosis and success. Well-illustrated with clinical photographs, radiographs, and diagrams, the book will enable practitioners to undertake endodontic retreatment with greater confidence.
- 89 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Clinical Success in Endodontic Retreatment
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Failures

Indications for Retreatment

Endodontic treatment should fulfill a variety of objectives (Schilder, 1967 and 1974):
• Create a continuously tapering preparation from the crown to the apices
• Maintain the position of the apical foramen on the root surface
• Maintain the shape of the original canal as much as possible
• Keep the apical foramen as small as possible
• Use copious irrigation to ensure the root canal system is thoroughly cleaned and disinfected
• Obturate and seal the root canal system.
Although the procedures for endodontic treatment of a vital or necrotic pulp were first described decades ago, the number of unsatisfactory endodontic results remains rather high. Epidemiologic studies published over the past 20 years show that the number of inadequate treatments varies between 60% and 79%, with a failure rate (that is, cases where clinical symptoms or periapical lesions exist) of 22 % to 63 % (Boucher et al, 2002).
Endodontic retreatment can be defined as further treatment performed because the initial treatment was inadequate or the lesion failed to heal.
From a clinical standpoint, the four causes of failure are inherent within each stage of endodontic treatment (Ruddle, 2004) :
• Inadequate access cavity due to failure to appreciate the anatomy of the tooth; this hampers visibility, which in turn results in the following:
– Failure to detect accessory canals
– Difficulty in correctly preparing the canal because of instruments further restricting visibility or difficulty in visualizing the entire canal system
– Perforations in the coronal third of the tooth or in the pulp chamber floor
• Insufficient irrigation during canal preparation
• Improper use of instruments during preparation, which may result in the following:
– Alteration of the canal trajectory, which can cause obstructions and eventual perforations
– Blockages and subsequent loss of working length (obstruction by debris or a fractured instrument); this prevents irrigation of the whole root canal system
– Widening of the apical foramen, making controlled obturation impossible
• An error in fitting the gutta-percha cone, resulting in moisture contamination, a fault frequently associated with inadequate preparation of the apex; however, obturation material extruded through the apex is not in itself an indication for either orthograde or retrograde retreatment.
From a biologic standpoint, endodontic failure can result from improper preparation, disinfection, or obturation of the root canal network. Reinfection of the canal system resulting from a poor coronal seal could also lead to endodontic failure.
Irrespective of the technical inadequacies or errors, all endodontic failures are directly associated with the presence of bacteria and their toxins in the root canal system; these irritants migrate into the periodontal tissues by any route possible (eg, apical foramen, lateral canals, accessory canals).
The goals of endodontic retreatment remain the same as the goals of the initial treatment: elimination of bacteria and prevention of further bacterial contamination by means of a well-obturated canal and a coronal seal. Achieving these goals ensures long-term success with little chance of relapse or reappearance of pathology (Figs 1-1a and 1-1b).

1-1a Preoperative periapical radiograph of a mandibular molar requiring endodontic retreatment prior to placement of a new crown.
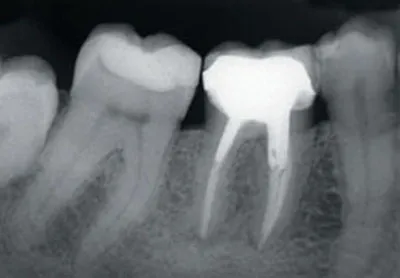
1-1b Periapical radiograph taken 9 years postoperatively. Good preparation and irrigation of the canal in conjunction with a good coronal seal ensures the longevity of the treatment.
Many endodontic failures can be attributed to inadequate training of the clinician and a lack of understanding of modern endodontic concepts and how to implement them. Resistance to change prevents many experienced practitioners from adopting new techniques, new instruments, and new materials; this, coupled with the misuse of unfamiliar equipment, contributes to a number of endodontic failures.
Endodontic treatment, when performed correctly, is predictable and enjoys a success rate above 95%. The same cannot be said for retreatment, in which access to canals can prove difficult, even dangerous, and in which negotiation of canals can be hampered by the following:
– Coronal restorations with large intracanal dowels
– Various canal filling materials such as hard and soft pastes, gutta-percha, or silver points
– Calcification of the apical portion of the canal as a result of inadequate preparation during initial treatment
– Iatrogenic causes including blockages, shoulders, ledges, perforations, and fractured instruments
Retreatment therefore necessitates the use of specific techniques and often proves complex and difficult.
When to Retreat?
A number of studies have shown that the decision to undertake endodontic retreatment is subject to both inter- and intrapractitioner variation. Agreement between practitioners on whether or not to retreat is rare (Aryanpour et al, 2000). The decision is often based on the individual practitioner’s personal criteria rather than on a set of universally recognized, objective criteria (Pagonis et al, 2000; Kvist and Reit, 2002).
Although it would be very difficult to produce universal guidelines to identify cases that should be retreated, a consensus does exist regarding certain situations that require endodontic retreatment (Friedman, 2002).
After rigorous clinical examination to eliminate any possible causes of failure that are nonendodontic in origin (eg, cracks or fractures, food packing, occlusal trauma, sinusitis, trigeminal neuralgia), endodontic retreatment should be undertaken in the following cases.
Clinical symptoms
Retreatment is indicated when clinical symptoms persist after initial treatment. Patients generally complain of spontaneous pain of variable intensity that is exacerbated by occlusal problems or during mastication. There may be signs of swelling, an abscess, or a fistula. Radiographic evidence of a lesion is not always present (Figs 1-2a and 1-2b).
At a clinical level, the following apply:
– Immediate postoperative pain...
Table of contents
- Cover
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- 1. Endodontic Failures and Indications for Retreatment
- 2. Removal of Existing Restorations
- 3. Access, Removal of Obturation Materials, and Negotiation of Canals
- 4. Management of Perforations
- 5. Treatment of Teeth with Open Apices
- 6. Prognosis and Retreatment
- Bibliography
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Clinical Success in Endodontic Retreatment by Stéphane Simon,Wilhelm-J. Pertot in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.