eBook - ePub
Flexible Bronchoscopy
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Flexible Bronchoscopy
About this book
In this fourth edition of the popular Flexible Bronchoscopy, which has been revised and updated throughout, the world's leading specialists discuss the technical and procedural aspects of performing diagnostic and therapeutic bronchoscopy. Four new chapters have been added, taking into account new developments in EBUS and electromagnetic navigation.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
A Short History of Flexible Bronchoscopy: From Fiberoptics to Robotics
Heinrich D. Becker
Department of Interdisiplinary Endoscopy, Thoraxclinic at Heidelberg University, Heidelberg, Germany
It is already 70 years since the beginning of bronchoscopic examination and the appearance of the flexible bronchofiberscope represents the opening of a new page in bronchoscopic examination. Future bronchoscopic examinations should make further progress on this milestone of the flexible bronchofiberscope.(Shigeto Ikeda [1])
1.1 Introduction
There is ample literature about the history of bronchoscopy in general. In this chapter, I will describe the steps that led to the development of the first flexible bronchoscope from prototype to the final device and the crucial steps of further evolution from fiberscopes to videoscopes, endobronchial ultrasound (EBUS) scopes, and the latest robotic flexible bronchoscope. The introduction of adjuvant technologies created a wide range of diagnostic and therapeutic applications for flexible bronchoscopy that has made it the central indispensible tool in pulmonary medicine today. I will describe how, driven by changing concepts, planned search for technical solutions or chance detection, new technologies were added to existing ones, leading to new concepts and strategies in a logical pattern. The examples given are early and advanced lung cancer, central airway obstruction, solitary pulmonary nodules (SPN), diseases of lung tissue, emphysema, and asthma. And finally, based on current developments I will take a look at the future of flexible bronchoscopy.
1.2 Shigeto Ikeda and the Invention of the Flexible Bronchoscope
From its introduction by Gustav Killian in 1897, the rigid bronchoscope remained the standard instrument for inspection of the airways during the following 70 years. Due to the comparatively complicated procedure, requiring special skills and in many cases additional general anesthesia, application of rigid bronchsocopy was mainly restricted to ENT departments, thoracic surgery, and specialized pulmonology centers. Only after Shigeto Ikeda introduced the flexible bronchoscope in 1967 did the art of bronchoscopy spread to many medical disciplines worldwide.
Ikeda was born in 1925 (Figure 1.1). After graduating from high school, he began studying medicine at Keio University in 1944. However, he had to interrupt his studies for one year as he suffered from specific pleuritis and underwent thoracoplasty. After recovery, he graduated in 1952 but in the same year, he had to have lung resection for a tuberculous mass during his internship in the Division of Tuberculous Surgery. Here he began studies on bronchial anatomy, including bronchography and motion pictures. As he found illumination by electric bulbs at the tip of rigid telescopes unsatisfactory, in 1962 he designed a telescope with “cold light.” A glass fiber bundle, connected to a 500 W xenon light source, was attached to the telescope and provided sufficient illumination for obtaining photographs and taking movies, for which he constructed special cameras.

Figure 1.1 Shigeto Ikeda, 1925–2001.
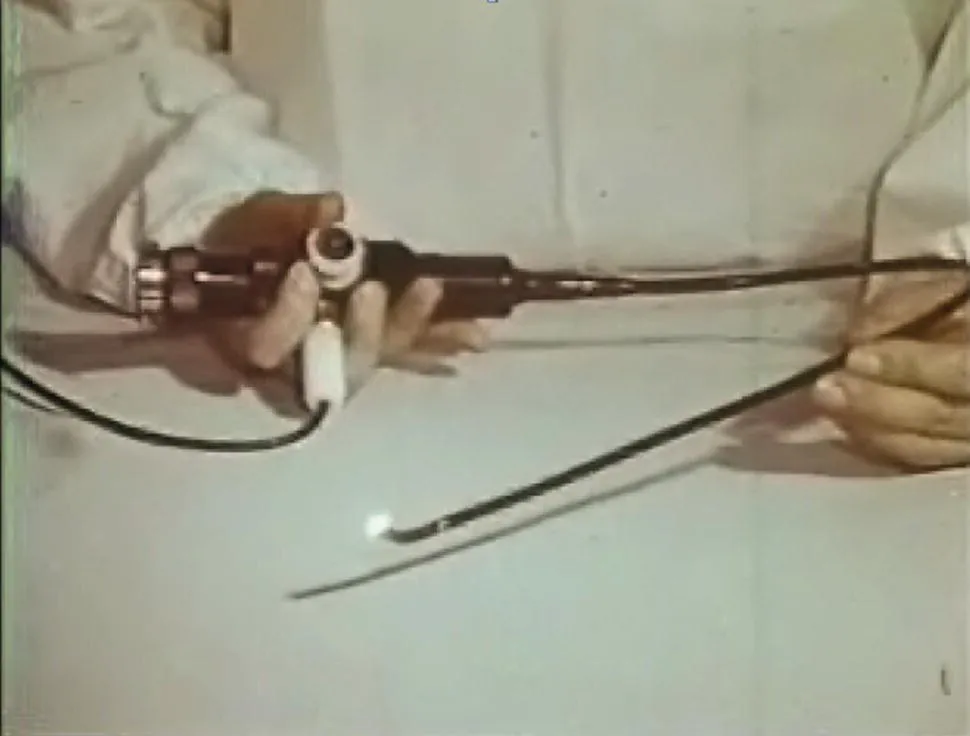
However, visualization of the bronchi in both upper lobes was often difficult due to the anatomical structures. Thus the need for a flexible bronchoscope, based on the concept of the gastrointestinal fiberscope presented by Basil Hirshowitz in 1961, was apparent [2,3]. As Machida Co. and Olympus Optical Co. had produced the first gastrofiberscopes in Japan from 1962, Ikeda approached Machida in 1964 and Olympus in 1965 for the construction of prototypes for bronchoscopy. He formulated specific requirements regarding diameter, more and smaller optical fibers, flexible light guide, fixed tip <1 cm, length 1 m, fixed focus 0.5–3 cm, visual angle 80°, and tip flexion of 60°. For ease of introduction, a special semiflexible orotracheal tube was constructed, that could be straightened in case specimens had to be obtained by a rigid forceps (Figure 1.2).

Figure 1.2 Ikeda demonstrating the first bronchoscope at my first visit to Japan. (Note: he was left handed, which is why the line to the light source and the suction of flexible bronchoscopes are running to the left so that the control section of the scope rests easily in your left hand and the lines are not pulling.) On the left is the first scope with the special orotracheal tube that could be straightened for taking rigid biopsies.
In 1966, when Ikeda presented the first prototype at the 9th International Congress on Diseases of the Chest in Copenhagen, Denmark, he created huge excitement and the story was even published in the New York Times. Further improvements were made on the following prototypes: control mechanisms for lengthwise rotation and bending of the tip were built into the control section, improved imaging was achieved by regular arrangement of smaller glass fibers, and a lens was mounted on the tip (Figure 1.3, movie). Finally, in the seventh prototype a channel was integrated into the scope for the introduction of sampling devices; Ikeda was confident that the instrument was ready for commercialization and introduced and popularized flexible fiberbronchoscopy throughout the world.
Source: Courtesy of T. Shirakawa.
In the following years, more and more experience was gained in clinical application and by 1980 flexible fiber bronchoscopy had become a routine procedure and spread worldwide. In 1980, after visiting Dumon in Marseille, Ikeda's group began Nd:YAG laser treatment and photodynamic therapy (PDT) of malignant lesions. For better image resolution and processing, ...
Table of contents
- Cover
- Table of Contents
- List of Contributors
- Preface
- About the Companion Website
- 1 A Short History of Flexible Bronchoscopy
- 2 Professor Ikeda's Genius
- 3 Applied Anatomy of the Airways
- 4 Infection Control and Radiation Safety in the Bronchoscopy Suite
- 5 Anesthetic Management for Diagnostic and Therapeutic Bronchoscopy
- 6 Indications and Contraindications in Flexible Bronchoscopy
- 7 Radial‐Probe Ultrasonography in Flexible Bronchoscopy
- 8 Convex‐Probe Ultrasonography in Flexible Bronchoscopy
- 9 Early Diagnosis of Lung Cancer
- 10 Electromagnetic Navigation Bronchoscopy
- 11 Virtual Bronchoscopic Navigation
- 12 Indirect Laryngoscopy
- 13 Bronchoscopy for Airway Lesions
- 14 Bronchoalveolar Lavage
- 15 Bronchoscopic Lung Biopsy
- 16 Transbronchial Needle Aspiration for Cytology and Histology Specimens
- 17 Staging of Bronchogenic Carcinoma
- 18 The Future of Interventional Pulmonology
- 19 Application of Laser, Electrocautery, Argon Plasma Coagulation, and Cryotherapy in Flexible Bronchoscopy
- 20 Flexible Bronchoscopy and the Application of Endobronchial Brachytherapy, Fiducial Placement, Radiofrequency Ablation, and Microwave Ablation
- 21 Foreign Body Aspiration and Flexible Bronchoscopy
- 22 The Role of Bronchoscopy in Hemoptysis
- 23 Endobronchial Stents
- 24 Balloon Bronchoplasty
- 25 Rigid Bronchoscopy
- 26 Pediatric Flexible Bronchoscopy
- 27 Bronchoscopy in the Intensive Care Unit
- 28 Bronchial Thermoplasty Management of Asthma
- 29 Endoscopic Management of Emphysema
- 30 Endoscopic Management of Bronchopleural Fistulas
- 31 Clinical Management of Benign Airway Stenosis and Tracheobronchomalacia
- Index
- End User License Agreement
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Flexible Bronchoscopy by Ko-Pen Wang, Atul C. Mehta, J. Francis Turner, Ko-Pen Wang,Atul C. Mehta,J. Francis Turner, Jr. in PDF and/or ePUB format, as well as other popular books in Medicine & Pulmonary & Thoracic Medicine. We have over 1.5 million books available in our catalogue for you to explore.