Gynaecological practice has changed fundamentally in the last three decades and a large proportion of major pelvic operations has been replaced by minimally invasive approaches. This book will cover minimally invasive approaches in all aspects of gynaecology including general gynaecology, oncology, urogynaecology and reproductive medicine. The chapters are written at a level appropriate for trainees/residents and general gynaecology specialists but enough details and additional resources will be provided for those who require further information. Specific aim of the book is to provide direct to the point surgical pearls which can be adapted to the daily practice instantly by the target audience.
The book includes chapters on relevant surgical anatomy, principles of MIS, management of camera systems, video/image editing, initiating a successful MIS practice, improving efficiency of current MIS program, how to develop successful teaching techniques in academic setting, avoiding & managing MIS related surgical complications and preoperative/postoperative care before covering MIS for individual conditions including intensive care managements. Chapters are written by world renown authorities.
ACOG guideline recently published a statement recommending vaginal hysterectomy and endoscopic hysterectomy should be considered as a first step of surgical choice. Current practice has been shifting from open cases to laparoscopic/ robotic assisted cases while vaginal cases stays steady. This shift has created an urge among gynaecologists to learn, improve or adapt laparoscopic/ robotic techniques in their practice.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
1 Practical fundamentals of retroperitoneal spaces for safe pelvic surgery: possible answers to difficult questions
MohamedMabrouk
DiegoRaimondo
ManuelaMastronardi
RenatoSeracchioli
1.1 Does a general gynecologist need to know about retroperitoneal pelvic anatomy ?
Separate works report a strong association between knowledge of pelvic anatomy and surgical competency [1]. The ability to manage several surgical procedures is -considerably influenced by the level of training in anatomy and the ability to identify key anatomical structures [2]. The importance of applied anatomy is suggested also by a 7-fold increase in claims made to the UK Medical Defence Organizations between 1995 and 2000 [3].
The most easily identifiable anatomical structures are pelvic organs and blood vessels. In contrast, retroperitoneum, nerves, and lymphatics are the least identifiable. Furthermore, whilst laparoscopy has become the standard of gynecological surgical care, the ability to identify pelvic structures at laparoscopy is found to be less than laparotomy [4].
Preliminary data of ongoing multicentric study conducted by Bologna University, assessing the necessity and level of training of retroperitoneal anatomy among gynecologists, have provided an overview of the poor knowledge and confidence of surgeons with this topic. Most of gynecologists sustain retroperitoneal anatomy as an essential topic in their work, but they perceive limitations in their anatomical knowledge and training.
Recognizing retroperitoneal structures is essential for the management of complex surgery (i.e., deep endometriosis, oncology) but can also be crucial for the so-called “everyday” surgery [5–7].
In this chapter, we aim to provide practical and basic knowledge of the retroperitoneal pelvic anatomy, referring to other chapters for the remaining anatomical topics.
1.2 What are the superficial anatomical landmarks of retroperitoneum?
Most pelvic organs are covered by the peritoneum, a serous membrane with openings at the lateral end of both uterine tubes. The peritoneum can be described in two parts: parietal peritoneum and visceral peritoneum. The parietal peritoneum is attached to the osteomuscular wall by extraperitoneal connective tissue; the visceral peritoneum, instead, is firmly adherent to the underlying viscera and often blends with connective tissue in the wall of the organs. The potential space between the two layers is called the peritoneal cavity.
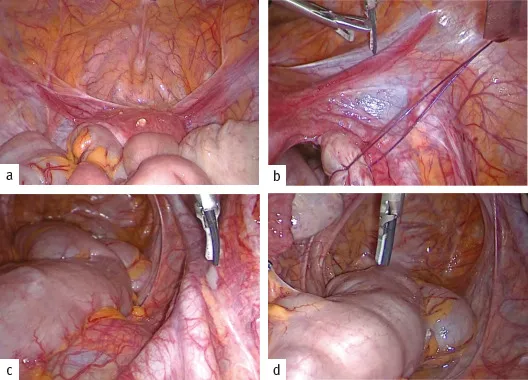
The peritoneum is reflected from the anterior and posterior uterine surfaces to the lateral pelvic wall forming the broad ligament of the uterus, which divides the pelvic cavity in the anterior and posterior compartments. Dorsally, the peritoneum covers the anterolateral surface of the upper rectum, a part of sacrum concavity and pelvic lateral walls, forming a retro-rectal peritoneal reflection. The presence of the uterus and the vagina produces two median pouches: the recto-uterine pouch (of Douglas) and the vesico-uterine (VU) pouch. It is important to note that the depth of the two pouches is variable and the peritoneal reflection of recto-uterine pouch of Douglas is more caudal than the VU one. Ventrally, the peritoneum that covers the dome of the bladder is reflected on the posterior surface of the lower anterior pelvic wall forming a prevesical reflection, when the bladder is empty (Fig. 1.1).
Fig. 1.1 Overview of the pelvis: (a) prevesical peritoneal reflection; (b) round ligament; (c) ureter at the pelvic brim and sacral promontory; (d) pouch of Douglas.
In patients with average weight, some retroperitoneal structures can be recognized through the peritoneum:
The peritoneum on the lower anterior abdominal wall is raised into five folds (reported as “ligaments”), which diverge as they descend from the umbilicus. They are the median, right and left medial, and right and left lateral umbilical folds.
The median umbilical fold extends from the apex of the bladder to the umbilicus and contains the urachus. The medial umbilical fold covers the obliterated umbilical artery. Under the lateral umbilical fold, the deep inferior epigastric vessels can be found, below their entry into the rectus sheath.
Superior vesical arteries, on both sides, form the transverse vesical folds on the bladders dome.
Uterine artery, on both sides, passes between the two peritoneal layers of the broad ligament, within the cardinal ligament (of Mackenrodt or lateral parametrium), and crossing over the ureter.
Pelvic ureter enters the lesser pelvis at the level of the sacral promontory, anterior to the end of the common iliac vessels (more frequent on the left side) or at the origin of the external iliac vessels (more frequent on the right side).
Uterosacral ligaments form the recto-uterine folds, containing some pelvic autonomic nerve fibers in its postero-lateral part. In some patients, it is also visible a more medial and caudal folder, enveloping the hypogastric nerves (HNs) and the inferior hypogastric plexus (or pelvic plexus) [8].
Bifurcation of aorta (at the level of the fourth lumbar vertebra or the L4/5 intervertebral disc, to the left of the midline) and the left common iliac vein. Middle sacral vessels and the superior hypogastric plexus are located in the interiliac triangle (or Cotte triangle) at the level of sacral promontory, the starting point of pelvic cavity.
Laterally, three somatic nerves from lumbar plexus: genitofemoral nerve lying on the psoas major muscle, and the iliohypogastric and the ilioinguinal nerves [9–11].
1.3 Is there a general scheme for the retroperitoneal space?
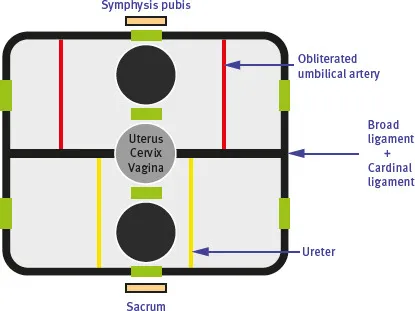
In the pelvis, three major layers can be identified: peritoneum; retroperitoneum, containing anatomical structures enveloped by connective tissue; and pelvic walls (muscles and bones covered by connective tissue). In a transversal section of the pelvis, it is possible to identify on the midline three main organs: bladder, cervix, and rectum (Fig. 1.2).
Fig. 1.2 General scheme of the retroperitoneum (the “exit doors” are represented by green boxes).
The functional organization of retroperitoneum (known as endopelvic fascia) is provided by dense connective structures—visceral “ligaments” and fasciae—leaving areas of looser connective tissue in contact with viscera and abdominal walls, forming spaces or septa (coalescence of fasciae). The method of dealing with these spaces represents the basis of retroperitoneal surgical dissection [12–15].
The endopelvic fascia has different characteristics according to its components, and it is divided into:
Membranous: parietal and visceral pelvic fasciae
The parietal pelvic fascia (PPF), which covers...
Table of contents
Title Page
Copyright
Contents
Copyright page
FOREWORD
Preface
Principal contributing authors
1 Practical fundamentals of retroperitoneal spaces for safe pelvic surgery: possible answers to difficult questions
2 Preoperative imaging for minimally invasive surgery in gynecology
3 Anesthetic considerations for minimally invasive surgery
4 Principles and safe use of electrosurgery in minimally invasive surgery
5 Laparoscopic entry techniques
6 Principles of laparoscopic suturing and alternatives
7 Challenges in minimally invasive surgery
8 Adhesions after laparoscopic and hysteroscopic surgery, prevention, and treatment
17 Robotic procedures for management of apical compartment prolapse
18 Laparoscopic management of mesh complications
19 Laparoscopic surgery for cervical cancer
20 Minimal invasive surgery for endometrial cancer
21 Minimally invasive surgery (MIS) for epithelial ovarian cancer (EOC)
22 Neuropelveology—the medicine of the pathologies of the pelvic nerves and plexuses
23 Complications of laparoscopic surgery and their management
24 Hysteroscopy: instrumentation for diagnostic and operative hysteroscopy, distension media, and office hysteroscopy
25 Hysteroscopic surgery for submucosal fibroids
26 Hysteroscopic surgery for Mullerian anomalies
27 Avoiding complications in hysteroscopic surgery
28 Endometrial ablation techniques for heavy menstrual bleeding
Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Minimally Invasive Surgery in Gynecological Practice by Ertan Saridoğan, Gokhan Sami Kilic, Kubilay Ertan, Gokhan Sami Kilic,Kubilay Ertan,Ertan Saridoğan in PDF and/or ePUB format, as well as other popular books in Medizin & Gynäkologie, Geburtshilfe & Hebammen. We have over 1.5 million books available in our catalogue for you to explore.