This companion to the popular book Practical Lessons in Endodontic Surgery offers expert guidance to clinicians who have limited experience in the nonsurgical procedures involved in root canal therapy. Synthesizing the latest clinical concepts and technologies with tried-and-true traditional treatment methods, it introduces readers to the challenges associated with nonsurgical endodontics and delivers realistic solutions in a clear, step-by-step, "lesson-based" format. Each of the 42 lessons offers useful, workable, and, above all, practical information and recommendations covering a specific aspect of endodontic care. Readers expand their knowledge incrementally, beginning with the essentials of patient diagnosis, examination, and record-keeping and progressing through lessons concerned with treatment planning and preparation for therapy; root canal instrumentation and obturation; and emergency and adjunctive procedures.
eBook - ePub
Practical Lessons in Endodontic Treatment
- 344 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Practical Lessons in Endodontic Treatment
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information

Medical Evaluation and Antibiotic Precautions
OBJECTIVE
To identify and respond to health issues that might compromise endodontic therapy.
OFFICE POLICY
A patient must complete a comprehensive medical/dental questionnaire before any dental treatment is initiated (Fig 1-1). It is the responsibility of the attending doctor to:
• Ascertain the responder’s authority to make the patient’s health care decisions if the responder to the questionnaire is someone other than the patient.
• Question the significance of all yes responses in the questionnaire.
• Ask the patient if any new medical problems have arisen since the last appointment.
• Verify the date of the patient’s last appointment. No questionnaire should be considered valid if 1 year or more has passed since the patient’s last appointment.
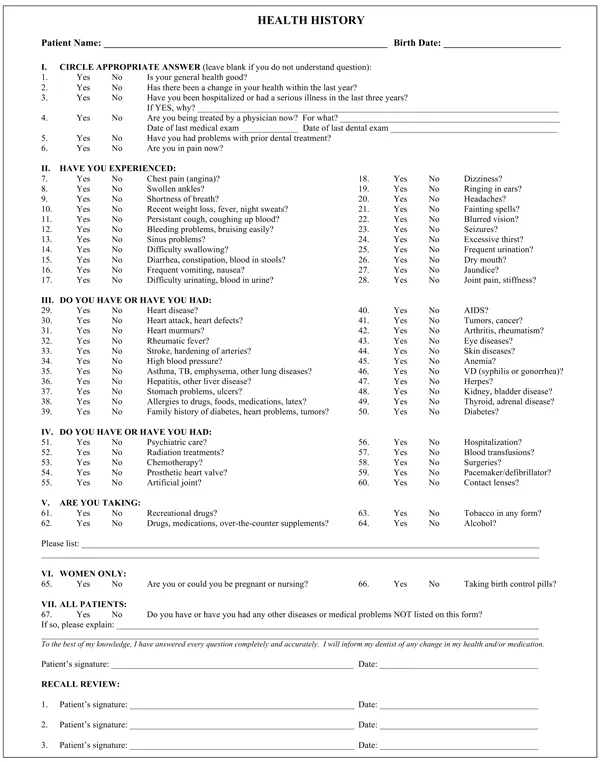
Fig 1-1 Example of a comprehensive Health History Form.
INACCURATE QUESTIONNAIRE
It is the responsibility of the attending doctor to be constantly aware of hidden signs of disease(s) that may be unknown to the patient or accidentally or intentionally withheld by the patient, such as:
• Fire red (flushed) or ashy pale (pallor) skin color and/or ankle and leg swelling that might indicate an undiagnosed cardiac problem, such as high blood pressure or congestive heart failure, or severe alcoholism.
• A yellowish or bronze skin color that might indicate liver, kidney, or endocrine impairment.
• Facial blemishes, gingival and/or palatal sores, and exposed needle marks that might indicate the patient is an alcohol or drug abuser and as such could be a carrier of hepatitis or a sexually transmissible disease.
• Facial varicosities that might indicate drug and alcohol abuse that could interfere with the dynamics (intensity and duration) of a local anesthetic.
Dentists should also be alert to patients seen on an emergency basis where the offending tooth has all the appearances of having been treated multiple times in the past, such as an excessively large endodontic access opening and overly aggressive canal enlargement. This may very well indicate that the patient is seeking emergency treatment only to acquire a prescription for pain medication. This situation is even more suspicious when the patient requests a specific pain medication.
Whatever the circumstances, a physician consultation request is always an option (see Physician Release Form, Fig 10-1).
RISK FACTOR CONCERNS
Based on the responses to both written and verbal questioning, patients should be mentally categorized into risk levels, and the treatment decision(s) should be based on the demands of that risk. The most serious and dangerous threat to a patient following a dental procedure is infective endocarditis (IE), which is more commonly called bacterial endocarditis.
Etiology
Bacteria enter the bloodstream (bacteremia), lodge on abnormal heart valves or other damaged heart tissue, and stimulate an infection of the inner lining of the heart. Only certain bacteria are prone to cause IE, and those microorganisms are normally found in the mouth and upper respiratory system.
Who is at risk
According to the American Heart Association (AHA), the American Dental Association (ADA), the Infectious Diseases Society of America (IDSA), and the Pediatric Infectious Diseases Society (PIDS), anybody is subject to IE, and IE is just as likely to occur from an everyday activity as it is from a dental procedure (AHA, Circulation, April, 2007).
Prevention
Use of a prophylactic regimen of antibiotics can help prevent IE.
Caution
According to the AHA, the risk of taking preventive antibiotics often outweighs the benefits. As such, the AHA does not recommend the injudicious use of broad prophylactic regimens of antibiotics for every patient.
The AHA conclusion
Prophylactic antibiotics should be reserved for moderate- to high-risk patients who might experience the gravest outcomes (eg, death) if left unprotected. The AHA guidelines are based on its comprehensive risk factor studies and are not intended to represent the standard of care for dentistry or to be a substitute for a dentist’s clinical judgment (Table 1-1).
| Table 1-1 | AHA recommendations of prophylactic antibiotic regimens for IE | |
| Situation | Agent | Regimen |
| Standard: For the general population | Amoxicillin | Adults: 2.0 g, children: 50 mg/kg Sig: orally 1 h before procedure |
| For patients unable to take medication orally | Ampicillin | Adults: 2.0 g, children: 50 mg/kg Sig: IM or IV 30 minutes before procedure |
| For patients with a penicillin allergy | Clindamycin | Adults: 600 mg Sig: orally 1 h before procedure |
| IM = intramuscular; IV = intravenous; Sig = write on label. | ||
RISK LEVELS
Negligible risks
The AHA does not recommend prophylactic antibiotics for patients that present to the office with the following conditions:
Cardiac conditions
• Repaired congenital heart defects
• Innocent heart murmurs
• History of rheumatic fever but no valve disease
• Coronary graft beyond a 6-month healing period
• Mitral valve prolapse, without valvar regurgitation
• Kawasaki syndrome, without valvar regurgitation
• A cardiac pacemaker/defibrillator (intravascular or epicardial)
Over-the-counter blood thinners
Patients taking over-the-counter blood thinners, such as aspirin, do not normally present a problem for routine endodontic procedures. Local coagulate methods, including pressure, epinephrine pellets (Epidri, Pascal), ferric sulfate products such as Stasis (Gingi-Pak) and Cuttrol (Icthys Enterprise), and calcium sulfate, are usually satisfactory in controlling hemorrhage even when the endodontic procedure involves a surgical intervention.
Pregnancy
• To avoid the possibility of inducing labor, endodontic care during the first trimester should be performed on an emergency basis only, and the treatment procedure and chair time at that appointment should be kept to a minimum.
• If the endodontic treatment is an elective procedure, it is wise to perform the service when the patient is in the second trimester.
• Antibiotics should be used sparingly, sedatives should be avoided, and the quantity of a vasoconstrictor used during treatment should be kept to a minimum.
Apprehension and anxiety
• Additional appointment time will be required to thoroughly explain the need and reasons for the endodontic procedure(s).
• Once it becomes apparent the patient is excessively fearful of the procedure, it is wise to suggest the use of a mild preoperative sedative.
• The use of rubber dam must be carefully and thoroughly explained, and to reduce the possibility of a sudden claustrophobic panic attack, the eyes and nose (airway) must be kept clear at all times.
• Though reassurance throughout the procedure will have a calming effect, the doctor and the assistant must be ever prepared for a patient’s sudden, even violent body and hand movements provoked by the stress of the procedure.
Neurologic issues
Epilepsy, palsy, Parkinson disease, facial and head tics, dementia, or the convulsive and/or emotionally disturbed patient.
• These patients are best served by prescribing appropriate preoperative sedatives or hypnotics, not prophylactic antibiotics.
• The doctor and assisting staff must be on constant alert for sudden patient movement(s) that could cause an inadvertent procedural accident.
• Referral is always an option.
Moderate risk
The AHA does recommend a prophylactic regimen of antibiotics for the following risk conditions:
Cardiac impairment ...
Table of contents
- Cover Page
- Cover Page
- Title Page
- Copyright Page
- Contents
- Contributors
- Preface
- PART ONE: Examination and Diagnosis
- PART TWO: Treatment Strategies and Decision-Making
- PART THREE: Preparation for Treatment
- PART FOUR: Canal Instrumentation: Shaping, Disinfection, and Case Management
- PART FIVE: Endodontic Obturation
- PART SIX: Emergency and Adjunctive Endodontic Procedures
- Suggested Readings
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Practical Lessons in Endodontic Treatment by Donald E. Arens,Alan H. Gluskin,Christine I. Peters,Ove A. Peters in PDF and/or ePUB format, as well as other popular books in Medicine & Dentistry. We have over 1.5 million books available in our catalogue for you to explore.