With ever-rising healthcare costs, evidence generation through Health Economics and Outcomes Research (HEOR) plays an increasingly important role in decision-making about the allocation of resources. Accordingly, it is now customary for health technology assessment and reimbursement agencies to request for HEOR evidence, in addition to data from clinical trials, to inform decisions about patient access to new treatment options.
While there is a great deal of literature on HEOR, there is a need for a volume that presents a coherent and unified review of the major issues that arise in application, especially from a statistical perspective. Statistical Topics in Health Economics and Outcomes Research fulfils that need by presenting an overview of the key analytical issues and best practice. Special attention is paid to key assumptions and other salient features of statistical methods customarily used in the area, and appropriate and relatively comprehensive references are made to emerging trends. The content of the book is purposefully designed to be accessible to readers with basic quantitative backgrounds, while providing an in-depth coverage of relatively complex statistical issues.
The book will make a very useful reference for researchers in the pharmaceutical industry, academia, and research institutions involved with HEOR studies. The targeted readers may include statisticians, data scientists, epidemiologists, outcomes researchers, health economists, and healthcare policy and decision-makers.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Data Sources for Health Economics and Outcomes Research
Kelly H. Zou, Christine L. Baker, Joseph C. Cappelleri, and Richard B. Chambers
CONTENTS
1.1Introduction
1.2Data Sources and Evidence Hierarchy
1.3Randomized Controlled Trials
1.4Observational Studies
1.5Pragmatic Trials
1.6Patient-Reported Outcomes
1.7Systematic Reviews and Meta-Analyses
1.8Concluding Remarks.
References
1.1Introduction
The health care industry and regulatory agencies rely on data from various sources to assess and enhance the effectiveness and efficiency of health care systems. In addition to randomized controlled trials (RCTs), alternative data sources such as pragmatic trials and observational studies may help in evaluating patients’ diagnostic and prognostic outcomes (Ford and Norrie, 2016). In particular, observational data are increasingly gaining usefulness in the development of policies to improve patient outcomes, and in health technology assessments (Alemayehu and Berger, 2016; Berger and Doban, 2014; Groves et al., 2013; Holtorf et al., 2012; Vandenbroucke et al., 2007; Zikopoulos et al., 2012). However, in view of the inherent limitations, it is important to appropriately apply and systematically evaluate the widespread use of real-world evidence, particularly in the drug approval process.
As a consequence of the digital revolution, medical evidence generation is evolving, with many possible data sources, for example, digital data from the government and private organizations (e.g., health care organizations, payers, providers, and patients) (Califf et al., 2016). A list of different types of research data, with their advantages and disadvantages, may be found in the Himmelfarb Health Sciences Library (2017), which is maintained by the George Washington University.
In this chapter, we provide a brief introduction of some common data sources encountered and analyzed in health economics and outcomes research (HEOR) studies, which include randomized controlled trials (RCTs), pragmatic trials, observational studies, and systematic reviews.
1.2Data Sources and Evidence Hierarchy
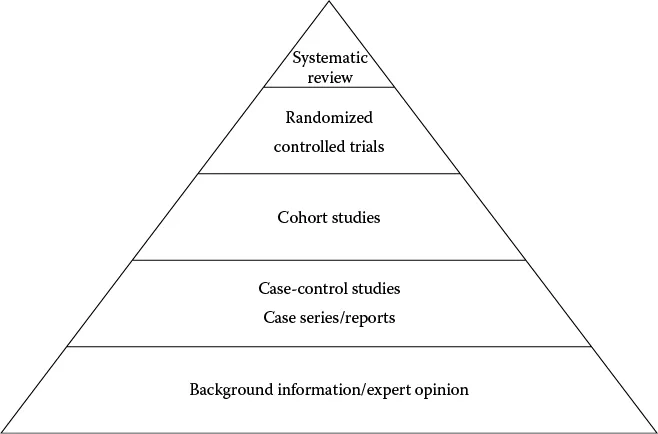
Murad et al. (2016) and Ho et al. (2008) provide the hierarchy or strength of evidence generated from different data sources. According to this hierarchy, depicted in the evidence pyramid in Figure 1.1, a systematic review/meta-analysis of randomized controlled trials (RCTs) and individual RCTs provides the strongest level of evidence, followed by cohorts, case-control studies, cross-sectional studies, and, finally, case series. In particular, prospective cohort studies are generally favored over retrospective cohort studies with regards to strength of evidence.
FIGURE 1.1 Evidence pyramid. (Modified from Dartmouth Biomedical Libraries. Evidence-based medicine (EBM) resources. http://www.dartmouth.edu/~biomed/resources.htmld/guides/ebm_resources.shtml, 2017.)
The Enhancing the QUAlity and Transparency Of health Research (EQUATOR) Network (2017) is an international initiative that seeks to improve the reliability and value of published health research literature by promoting transparent and accurate reporting and a wider use of robust reporting guidelines. It is the first coordinated attempt to tackle the problems of inadequate reporting systematically and on a global scale; it advances the work done by individual groups over the last 15 years. The EQUATOR’s (2017) website includes guidelines for the following main study types: randomized trials, observational studies, systematic reviews, case reports, qualitative research, diagnostic/prognostic studies, quality improvement studies, economic evaluation, animal/preclinical studies, study protocols, and clinical practice guidelines.
1.3Randomized Controlled Trials
The RCT was first used in 1948, when the British Medical Research Council (MRC) evaluated streptomycin for treating tuberculosis (Bothwell and Podolsky, 2016; Holtorf, 2012; Sibbald and Roland, 1998). A well-conducted RCT design is generally considered to be the gold standard in terms of providing evidence, because causality can be inferred due to the design’s comparisons of randomized groups that are balanced on known and unknown baseline characteristics (Bothwell and Podolsky, 2016). In addition, RCT studies are conducted under controlled conditions with well-defined inclusion and exclusion criteria. Hence, RCTs are the strongest in terms of internal validity and for identifying causation (i.e., making inferences relating to the study population).
Frequently, a placebo group serves as the control group; however, the use of an active control, such as standard of care, is becoming more common. The expected difference on the primary outcome of interest between the interventional group(s) and the control group is the central objective. Typical endpoints include the mean change from baseline, the percent change, and the median time to an event, such as disease recurrence.
A double-blind design is often used in RCTs of pharmaceutical interventions, where assignments into the intervention and the control groups are not known in advance by both investigators and patients. This methodological framework minimizes possible bias that might result from awareness of the treatment group.
According to the Food and Drug Administration (FDA, 2017), the numbers of volunteers across several phases of RCTs are as follows: Phase 1: 20 to 100; Phase 2: several hundred; Phase 3: 300 to 3000; and Phase 4: several thousand. Further details about these phases are also described.
In addition, according to the National Library of Medicine’s (NLM, 2017) clinical trial registration site, ClinicalTrials.gov, there are five phases of clinical trials involved in drug development. Phase 0 contains exploratory studies involving very limited human exposure to the drug, with no therapeutic or diagnostic goals (e.g., screening studies, micro-dose studies). Phase 1 involves studies that are usually conducted with healthy volunteers, and emphasize safety. The goals of Phase I studies are to find out what the drug's most frequent and serious adverse events are and, often, how the drug is metabolized and excreted. Phase 2 includes studies that gather preliminary data on efficacy (whether the drug works in people who have a particular disease or condition under a certain set of circumstances). For example, participants receiving the drug may be compared with similar participants receiving a different treatment, usually an inactive substance, called a placebo, or a standard therapy. Drug safety also continues to be evaluated in Phase 2, and short-term adverse events are studied.
Phase 3 includes confirmatory studies for the purpose of regulatory approval and gather more information about the efficacy and safety by studying targeted populations, with possibly different dosages and drug combinations. These studies are typically much larger in size than the Phase 2 studies, and are often multinational. Phase 4 contains studies that occur after the Food and Drug Administration (FDA) has approved a drug for marketing. These studies involve a postmarket investigation to sponsored studies required of or agreed to by the study sponsor for the purpose of gathering additional information about a drug's safety, efficacy, or optimal use scenarios, including its use in subgroups of patients.
The numbers of volunteers were as follows: Phase 1: 20 to 100; Phase 2: several hundred; Phase 3: 300 to 3000; and Phase 4: several thousand (https://www.fda.gov/ForPatients/Approvals/Drugs/ucm405622.htm#Clinical_Research_Phase_Studies).
Over the last few decades, the use of a particular type of RCT—the multicenter clinical trial—has become quite popular. As a result of a potentially long enrollment period, trial enrollment may benefit from simultaneous patient recruitment from multiple sites, which may be within a country or region. Pharmaceutical and biotechnology companies and parts of the US National Institutes of Health (NIH), such as the National Cancer Institute, have been among the sponsors of multicenter clinical trials. Such large and complex studies require sophisticated data management, analysis, and interpretation.
ClinicalTrials.gov of the US NLM (2017) is a registry and results database of publicly and privately supported clinical studies of human participants that have or are being conducted around the world. It allows the public to learn more about clinical studies through information on its website and provides background information on relevant history, policies, and laws. In April 2017, this website listed approximately 240,893 studies with locations in all 50 US states and in 197 countries. According to the displayed enrollment status, the locations of recruiting studies are as follows: non-US-only (56%), US-only (38%), and both US and non-US (5%). Thus, most of the registered studies are conducted outside of the United States.
It is noted that RCTs are compromised with respect to external validity (i.e., making inferences outside of the study population or testing conditions), since the conditions under which they are conducted do not necessarily reflect the real world, with its inherent complexity and heterogeneity. Accordingly, data from nonrandomized studies may need to be used to complement RCTs or to fill the evidentiary gap created by the unavailability of RCT data.
1.4Observational Studies
Section 3022 in the 21st Century Cures Act of the United States Congress (United States Congress, 2016) defines the term “real-world evidence” (RWE) to mean “data regarding the usage, or the potential benefits or risks, of a drug derived from sources other than randomized clinical trials.” Accordingly, noninterventional (observational) studies do not involve randomizations, but can provide real-world data (RWD) to generate RWE. Such studies are selected due to their ease of implementation, cost considerations, and generalizability from broad experiences (Garrison, 2007). Sherman et al. (2016) indicate RWE includes “information on health care that is derived from multiple sources outside typical clinical research settings, including electronic health records (EHRs), claims and billing data, product and disease registries, and data gathered through personal devices and health applications.”
RWD generally represent the various complex treatment choices, switches between the treatments, the strengths (dose levels), and the days of supply (pill counts) that are often found in actual clinical practice. Furthermore, adding patients’ demographic characteristics, comorbidities, concomitant treatments, and switches between therapies provides a real-world understanding of the magnitude and variability of the treatment’s effect in different sets of circumstances.
Observational studies involve existing databases, with standardized methodologies employed depending on the objective of the question being evaluated. Use of this methodological framework can be both practical and convenient and, in addition, prospective or retrospective. Cohort studies, cross-sectional studies, and case-control studies are among the different types of study designs included within the umbrella of observational studies (...
Table of contents
Cover
Half Title
Series Page
Title Page
Copyright Page
Table of Contents
Preface
Acknowledgment
About the Editors
Authors’ Disclosures
1. Data Sources for Health Economics and Outcomes Research
2. Patient-Reported Outcomes: Development and Validation
3. Observational Data Analysis
4. Predictive Modeling in HEOR
5. Methodological Issues in Health Economic Analysis
6. Analysis of Aggregate Data
7. Health Economics and Outcomes Research in Precision Medicine
8. Best Practices for Conducting and Reporting Health Economics and Outcomes Research
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Statistical Topics in Health Economics and Outcomes Research by Demissie Alemayehu, Joseph C. Cappelleri, Birol Emir, Kelly H. Zou, Demissie Alemayehu, PhD,Joseph C. Cappelleri, PhD,Birol Emir, PhD,Kelly H. Zou, PhD, Pstat,Demissie Alemayehu,Joseph C. Cappelleri,Birol Emir,Kelly H. Zou, Demissie Alemayehu, PhD, Joseph C. Cappelleri, PhD, Birol Emir, PhD, Kelly H. Zou, PhD, Pstat in PDF and/or ePUB format, as well as other popular books in Economics & Pharmaceutical, Biotechnology & Healthcare Industry. We have over 1.5 million books available in our catalogue for you to explore.