![]()
Multidrug resistance-1 gene variants in pediatric leukemia in Bali
R. Niruri, N.L. Ulandari & S.C. Yowani
Department of Pharmacy, Faculty of Mathematics and Science, Udayana University, Bali, Indonesia
I. Narayani
Department of Biology, Faculty of Mathematics and Science, Udayana University, Bali, Indonesia
K. Ariawati
Division of Hematology Oncology, Department of Pediatrics, Sanglah Hospital, Bali, Indonesia
ABSTRACT: Variants of the Multidrug Resistance-1 (MDR1) gene play an important role in chemo-resistance in Acute Lymphoblastic Leukemia (ALL). In this study, we aimed to identify MDR1 gene variants 3435 and 2677 in children with ALL in Sanglah Hospital, Bali, and to determine their chemo-therapeutic outcome. All children with ALL admitted in Sanglah Hospital during May 2015 to January 2016 were included. The PCR method was used to identify the MDR1 gene. Remission status was determined after the induction phase of Indonesian Protocol ALL 2006. The sequencing results from 17 patients indicated that four children had mutations 3435T and 2677T, two possessed mutation 3435T and wild-type 2677G, and the remaining had wild-type 3435C and 26TTG. Of those 17 children, 16 were able to continue with the same chemotherapy protocol and had complete remission.
1 INTRODUCTION
Acute lymphoblastic leukemia (ALL) is the most frequently detected cancer in children worldwide (Zhai 2012) as well as the highest reported type in Department of Pediatric Hematology-Oncology, Sanglah Hospital, Bali (Mudita 2007). Multid-rug resistance-1 (MDR1) gene-encoded P-glyco-protein (P-gp) plays a role in drug resistance. It is able to pump out the drugs (e.g., vinca alkaloids, steroids, and anthracyclines) from the intracellular cytoplasm (Calado 2002, Wuchter 2000). P-gp overexpression exists in neoplastic cells, so it can deteriorate the therapeutic results and worsen prognosis (Li 2006, Leith 1999). The expression on leukemic cells is associated with chemotherapy resistance (Calado 2002, Wuchter 2000). The variation of P-gp expression is determined by the gene (Calado 2002). The differences in the frequencies of MDR1 gene polymorphisms are influenced by ethnic groups (Gregers 2015, Jamroziak 2005, Li 2006), which could be considered as a possible reason for different findings (Li 2006, Schwab 2003). Single-nucleotide polymorphisms (SNPs) at position 3435C > T (exon 26) and position 2677 G > T (exon 21) occur frequently (Fung 2009, Brambila-tapia 2013).
In this study, we aimed to identify variants 3435 and 2677 of the MDR1 gene in children with ALL in Sanglah Hospital, Bali, and to determine the chemotherapy results.
2 METHODS
This study was approved by Medical School, Udayana University, Sanglah Hospital ethical committee and conducted in Sanglah Hospital and Biology Molecular Laboratory, Faculty of Medical School, Udayana University. All children (0 to 12 years old) with ALL in Sanglah Hospital in the period of May 2015 to January 2016 who signed informed consent form were included in this study.
Buffy coat samples obtained from the patients’ whole blood or bone marrow aspiration were stored in –80°C. Deoxyribonucleic acid (DNA) was isolated from buffy coat with a standard salting out protocol. The primers to determine variant 3435 were 5’ACT CTTGTTTTCAGCTGCTTG 3’ (forward (F)) and 5’CATTAGGCAGTGACTCGATG 3’ (reverse (R)), producing 206 base pairs (bp) polymerase chain reaction (PCR) product (Miladpour 2009), and the primers for 2677 were 5’TATCCTTCATCTATGGTTGG 3’ (F) and 5’TTTAGTTTGACTCACCTTCCC 3’(R) (Huang 2005), yielding 155 bp product. PCR amplification was initiated with 5 min pre-denaturation at 94°C, which was followed by 35 cycles of denaturation (94°C, 90), annealing at 56°C (for 3435 SNP) and 48°C (for 2677, 60 s), and extension (72°C, 60 s). The final extension was at 72°C for 10 min. The PCR products were identified by electrophoresis in a 1.5% agarose gel that was stained with 0.5 μg/ml of ethidium bromide, and then visualized under a UV transilluminator. The remaining PCR products of each variant in exon 26 and 21 were sequenced and compared with the sequence of the wild-type (WT) MDR1 gene (Chen 1990).
All the patients received chemotherapy Indonesian Protocol ALL 2006 standard risk (SR) or high risk (HR). The chemotherapeutic response was based on remission status after induction phase. Data of complete remission (CR) achievement were collected from medical records. P-gp expression data were documented from our previous study with flow cytometry (Niruri 2017).
3 RESULTS AND DISCUSSION
On the basis of sequencing result from 17 patients (Table 1, Figures 1 and 2), 4 had mutations 3435T and 2677T, 2 possessed mutation 3435T and wild-type 2677G, and the remaining children had wild-type 3435C and 2677G. In this study, there was no patient with 2677G > A. The frequency of 2677G > T was much higher than 2677G > A (Fung 2009). Because of cell viability and availability of reagents in our previous study (Niruri 2017), not all the patients exhibited P-gp expression (Table 1).
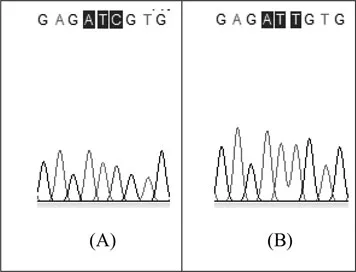
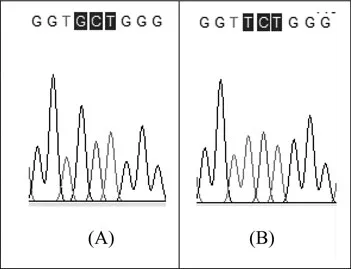
The 3435 C > T (Figure 1) is a synonymous SNP, but it can alter mRNA level, protein folding to substrate specificity, and protein expression. Several studies have been conducted to identify the effect of the presence of variant 3435 and its haplotype on MDR1 structure and function. Some possibilities have been reported. First, stability of MDR1 mRNA was altered by the mutation (Fung 2009, Hoffmeyer 2000, Kimchi-Sarfaty 2007). Second, kinetics in translation can be altered by the use of a rarer codon (Fung 2009, Kimchi-Sarfaty 2007). It can alter the dynamics of protein folding. Synonymous polymorphism could result in ribosome stalling (Fung 2009, Tsai 2008). Nucleotide mutation can change the mRNA structures, which eliminate or generate new secondary structures (e.g., pseudoknot or hairpin). These changes can delay the ribosome and alter translation (Fung 2009). The 3435 C > T may interfere in co-translational folding in close amino acids (which are 30–72 codons in front of the mutant codon). The site of 3435 C > T is in the second ATP-Binding domain. The alteration on pause signal may affect the folding of Q-loop and walker-A motifs. Therefore, it can change MDR1 function such as by altering ATP-binding affinity or ability of ATP hydrolysis (Fung 2009). Meanwhile, another variant, the 2677 G > T (Figure 2), is a non-synonymous SNP. A change in the nucleotide sequence at position 2677 can cause a ribosome pause, which may alter the co-translation of amino acids, which are before the transmembrane domains (TM) 6 and TM 10 (Fung 2009, Sakurai 2007). Each allele that makes haplotype can produce a small but significant, synergistic, or additive change contribution to alter protein folding, function, and expression (Fung, 2009, Kim, 2006). Therefore, it can affect the disposition of chemotherapy drugs (Kim 2006).
Table 1. Remission status of the patients with MDR1 gene variants 3435 and 2677 (Ntotal = 17).
| n (Nucleotide sequence of the MDR1 gene at positions 3435/2677) |
SR/HR | 3435 (Mut)/2677(Mut) | 3435(Mut)/2677 (Mut) | 3435(WT)/2677 (WT) | CR |
SR | 2** (gagatTgtg / ggtTctggg) | 1* (gagatTgtg / ggtGctggg) | 6 (gagatCgtg / ggtGctggg) | CR |
HR | 1** (gagatTgtg / ggtTctggg) | 1* (gagatTgtg / ggtGctggg) | 5 gagatCgtg / ggtGctggg) | CR |
SR → HR | 1** (gagatTgtg / ggtTctggg) | – | – | CR* |
Total | 4 | 2 | 11 | 17 |
Mut: mutant; WT: wild-type; CR: complete remission; SR/HR: standard risk or high risk; SR → HR: a switch protocol (from SR to HR) after the window phase of the induction course; (*): CR was achieved after the protocol was changed; (**): all the mutants have P-gp overexpression based on our previous study on P-gp expression in patients with ALL.
Figure 1. Patients’ MDR1 sequence at position 3435: (A) wild-type sequence and (B) variant 3435C > T.
Figure 2. Patients’ MDR1 sequence at position 2677: (A) wild-type sequence and (B) variant 2677G > T.
There were discrepancies among the studies of the MDR1 gene and chemotherapeutic responses. In acute myeloid leukemia (AML), the wild-type variants, a CC genotype at position 3435 and a GG genotype at position 2677, had higher probability to achieve CR and maintain 3-year event-free survival (EFS) than non-CC genotype at 3435 and non-GG genotype at 2677. The CC and GG genotypes were significantly related to a reduced expression of P-gp. Therefore, it could increase intracellular accumulation of the drugs. The influence of variants 3435 and 2677 on CR achievement might depend on the chemotherapeutic agents used in the induction course (Kim 2006). Haplotypes contribute to medication therapy outcome and disease susceptibility (Fung 2009). In this study, 16 out of 17 patients showed CR after induction phase, and the remaining 1 patient who had variants 3435 C > T and 2677 G > T must switch from standard-risk protocol to high-risk protocol to get CR (Table 1). A similar result was also found in a study conducted by Jamroziak (2005). Adult patients who were diagnosed with ALL with different MDR1 genotypes at 3435 showed a similar probability of achieving CR after the first induction phase (Jamroziak 2005). However, 3435 C > T was significantly related to risk of relapse (Jamroziak 2005, Gregers 2015). Adverse events on bone marrow during prednisolone, vincristine, and doxo rubicin in the induction course were more prominent in childhood ALL with 3435 TT than other genotypes (Gregers 2015). The effects of haplotype on therapeutic outcome, toxicity, and survival rate need to be explored in future studies.
One patient with 3435C > T and 2677G > T SNPs showed prednisone poor responders on window phase at induction of SR protocol (Table 1). In the ALL trial, patients with poor response after prednisone therapy had lower estimated EFS than those with good response (Bhojwani 2009). The patients’ protocol was switched to Indonesian Protocol ALL 2006 of HR group to get CR (Table 1). T-cell phenotype associated with a poor prednisone response was reported (Bhojwani 2009). Some possible mechanisms of reversal resistance by steroid switch occur, which would give a better response in cancer (Lorente 2014). On some trials, dexamethasone showed greater activity than prednisone in killing lymphoblast and in reducing the occurrence of central nervous system involvement because of higher level of free-drug and higher ability to pass through the blood–brain barrier (Balis 1987, Ito 1996, Mitchell 2005). However, adverse events occurred more frequently with dexamethasone than with prednisone (Belgaumi 2003, Hurwitz 2000, Mitchel 2005). Polymorphisms on glucocorticoid pathway genes e.g., MDR1 gene and NR3C1) were also significantly associated with hormone concentration and pharmacokinetic parameters (Nebesio 2016). All four patients in this study with mutants at position 3435 and/or 2677 showed P-gp overexpression, but different therapeutic responses (Table 1). More than 50 SNPs of the MDR1 gene have been reported on the National Center for Biotechnology Information (Fung 2009). The MDR1 gene variant 1236C > T was related to the treatment response of steroid in the idiopathic nephrotic syndrome (NS) (Safan 2016). A higher frequency of 1236C > T was found in late responders to pre...