- 612 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Autonomic Pharmacology
About this book
This overview of autonomic pharmacology describes the anatomy, physiology and pharmacology of the autonomic involuntary nervous system. Covering the diverse group of drugs acting on the autonomous nervous system, their actions are reviewed together with their clinical uses, side effects, interactions and subcellular mechanisms of action. Information is organized in a logical flow, bringing together the latest advances in an integrated form on topics usually found only in a fragmented form.; This work is intended for all those researching in industry and academic institutions in pharmaceutical, pharmacological sciences, pharmacy, medical sciences, physiology, neurosciences, biochemistry and molecular biology.
1
Anatomy and Physiology of the Autonomic Nervous System
1.1 Introduction
1.2 Smooth Muscle
1.2.1 Single-unit Smooth Muscle
1.2.2 Multi-unit Smooth Muscle
1.3 Structure of Autonomic Nerves
1.4 Structure of the Autonomic Nervous System
1.5 The Efferent Autonomic Pathways
1.5.1 Sympathetic pathways
1.5.2 The adrenal medullae
1.5.3 Parasympathetic pathways
1.5.4 The Enteric Nervous System
1.5.5 Summary of Efferent Autonomic Pathways (Fig. 1.6)
1.6 Physiological Responses of the Innervated Organs to Autonomic Nerve Stimulation
1.6.1 The Eye
1.6.2 Salivary Glands
1.6.3 Lacrymal Glands
1.6.4 Thyroid Gland
1.6.5 Heart
1.6.6 Blood Vessels
1.6.6.1 Coronary circulation
1.6.7 Skin
1.6.8 Lungs
1.6.9 Gastrointestinal Tract
1.6.10 Liver
1.6.11 Pancreas
1.6.12 Gall Bladder and Bile Duct
1.6.13 Spleen
1.6.14 Kidneys
1.6.15 Urinary Bladder
1.6.16 Genital Tract
1.6.17 Adipocytes
1.7 Afferent Sensory Pathways
1.7.1 Spinal Reflexes
1.7.2 Medullary Reflexes
1.7.2.1 Cardiovascular reflexes
1.7.2.2 Respiratory reflexes
1.7.2.3 Swallowing and vomiting reflexes
1.7.3 Midbrain
1.7.4 Hypothalamus
1.7.5 Thalamus
1.8 Efferent Functions of Afferent Neurones
1.9 Relationships Between Higher Centres and Autonomic and Somatic Nervous Systems
1.10 Considerations in the Classification of Autonomic Nerve Pathways
1.1 Introduction
The autonomic nervous system controls the internal involuntary functions of the body. These are the functions concerned with the maintenance of a constant internal environment, that is, homeostasis. The major activities and systems under the control of the autonomic nervous system include digestion, the cardiovascular system (such as the blood pressure), blood chemistry, breathing and body temperature. Control of these functions is below the level of consciousness, hence the term involuntary nervous system. The major cellular structures that are innervated by the autonomic nervous system are smooth muscle, cardiac muscle, glandular tissue and adipocytes (fat cells). Thus, the digestion of food occurs by the secretion of digestive enzymes from the intestinal glands of the intestinal mucosa and rhythmic contraction and relaxation of circular and longitudinal smooth muscle arranged in the intestinal wall propels the chyme along and chums it up to aid digestion. We are unaware of this process and have little conscious control over it. The autonomic nervous system modulates this digestive activity by either speeding or attenuating.
The autonomic nervous system has been subdivided into the sympathetic and parasympathetic systems based upon their physiological functions and their anatomy. The word ‘sympathetic’ is derived from the term nervi sympathici majores used by Winslow (1732) to describe the nerves which he thought carried out ‘sympathies’ and co-ordinate various visceral functions. The sympathetic nervous system is concerned with adaption to stressful situations, which Cannon (1929) described as preparing the body for ‘flight and fight’. In contrast, the parasympathetic division’s role is to conserve and restore energy. Thus, in general they have opposing actions upon tissues, the heart being a good example. The rate and force of cardiac contractions are elevated by an increase in sympathetic nerve discharge in response to a stressful stimulus. In contrast, raised parasympathetic nerve activity to the heart causes slowing. Digestion is a function not essential for survival of immediate danger and is therefore retarded by sympathetic nervous activity, whereas parasympathetic activity stimulates digestion during rest and recovery from stress.
The role of the autonomic nervous systems in controlling smooth muscle activity differs from that of the somatic nervous system which is responsible for the contraction of skeletal (striated, voluntary) muscle. The contraction of mammalian skeletal muscle depends almost entirely upon the arrival of a nerve impulse along the somatic nerve and release of the neurotransmitter, acetylcholine (Ach). If the somatic nerve is destroyed, then the muscle becomes paralysed and eventually atrophies. In contrast, smooth muscle continues to function in the absence of an autonomic innervation but without its modulating influence.
A feature common to both the autonomic and somatic nervous systems is that both operate as a reflex arc. Some authorities regard the autonomic nervous system solely as an efferent system carrying motor impulses to the smooth muscle. However, afferent fibres dispatch sensory information regarding the body’s internal environment via autonomic or somatic nerves to the central nervous system (CNS) where it is integrated before efferent impulses are sent to the effector organ. In this book, the autonomic nervous system is regarded both as an afferent and efferent system, since it is important to understand the autonomic reflexes when considering the pharmacology of drugs acting on the autonomic nervous system and its effectors. Furthermore, the sensory nerves are increasingly being recognized as sites of drug action in their own right.
Unlike the efferent somatic nerves which leave the spinal cord and pass directly to the skeletal muscle, autonomic efferents synapse once outside the spinal cord or brain stem before arriving at the innervated smooth muscle. These synapses occur with groups of cell bodies which are the autonomic ganglia.
1.2 Smooth Muscle
Smooth muscle fibres are arranged in sheets in the walls of the hollow organs such as the intestine and bladder. The individual fibres may be arranged in parallel, such as in the longitudinal muscle layer of the intestine which surrounds an inner circular muscle layer. In other organs, such as the uterus and bladder, the fibres form a network in which they run randomly in different directions. Smooth muscle has been classified by Bozler (1948) into two types: single-unit and multi-unit muscle (Figure 1.1).
1.2.1 Single-unit Smooth Muscle
The individual muscle cells are arranged so that adjacent fibres are in contact with each other through specialized gap junctions, which allows the spread of a wave of contraction throughout the muscle. The point of contact probably provides a low resistance pathway for ephaptic transmission, whereby local circuit currents are set up between adjacent cells. Chemical or mechanical transmission between smooth muscle cells is unlikely to occur.
The muscles develop tone or display rhythmic contractile activity. This tone or myogenic activity is not dependent upon the presence of the autonomic nerves but the nerve impulse to the smooth muscle modifies this activity either by increasing or decreasing the magnitude of contractions and their frequency. Not all fibres of single-unit smooth muscle may receive an autonomic innervation, but its influence will spread readily to adjacent fibres. Single-unit smooth muscle does not respond to single electrical stimuli of the innervating nerves, although a small depolarization of each cell membrane occurs. With trains of stimuli, depolarizations summate to finally induce an action potential and contraction of the muscle.
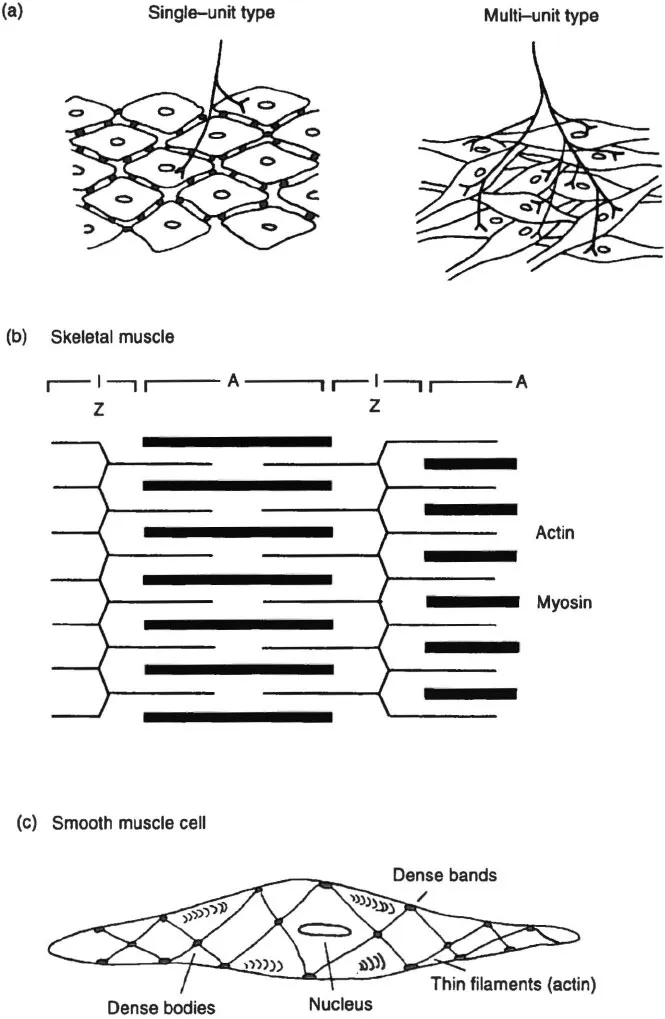
Figure 1.1 (a) Arrangement and innervation patterns of smooth muscle cells of the single-unit and multi-unit types. (b) Contractile filaments arrangement in skeletal muscle showing the A and I bands and the Z line forming the point of attachment of actin myofilaments. (c) A smooth muscle cell showing contractile myofilaments and their points of attachment to the cell membrane at dense bodies.
The membranes of smooth muscle cells are polarized, the inside being negative with respect to the outside. The resting membrane potential is ∼60 mV. This is due to the combined effects of the sodium pump which expels Na+ from the cell, the relatively greater permeability of the cell membrane to K+ which reaches a higher concentration on the inside of the cell, and to the presence of large organic anions on the inside of the cell. Reduction of the resting membrane potential to a critical level generates a propagated action potential whereby the membrane is depolarized and contraction ensues.
The spontaneous rhythmic activity of smooth muscle is generated by pacemaker potentials or slow depolarizations of the cell membrane. These have been classified by Kuriyama (1970) into three types.
1 Type I. A slow potential of short duration acting as a prepotential for an individual spontaneous spike. These may be due to oscillations in internal Ca2+ concentration, [Ca]i (Tomita & Watanabe 1973).
2 Type II. An excitatory potential generated by nervous activity which may occur at a local level. For example, the intramural plexus of the intestine contains a local nerve loop triggered by a rise in intraluminal pressure (see later). This is therefore neurogenic in origin and responsible for peristalsis.
3 Type III. Slow depolarization leading to a train of spike discharges and known as slow waves. Each depolarization and train of superimposed spikes is accompanied by a contraction of the muscle. The frequency ranges from 1 to 18 per minute in different muscles. Their generation and propagation are not prevented by tetrodotoxin (TTX), the inhibitor of Na+ channels in excitable cells, with specificity for nervous tissue. Slow waves are not therefore neurogenic but myogenic. The frequency of myogenic activity is increased by stretching. Slow waves and spontaneous tone are often abolished by indomethacin, an inhibitor of cyclo-oxygenase, and are therefore attributed to endogenous arachidonic acid products (eg guinea-pig tracheal and intestinal smooth muscle) (Tomita 1989).
Special pacemaker cells may lie between longitudinal and circular muscle layers of the gastrointestinal tract. They may affect both layers equally, or one layer more than the other depending on species and location. Slow waves in the region of highest frequency will drive cells in neighbouring areas. In some tissues the pacemaker is in a fixed position, for example, in the ureter it is at the end nearest the kidney. In other tissues it may vary as different regions have the highest frequency. Smooth muscle slow waves consist of an initial component which is probably the driving force originating in specialist pacemaker cells, followed by a secondary component with superimposed spike potentials. These latter two aspects are probably due to Ca2+ influx, since they are abolished by the calcium channel antagonists, verapamil and nifedipine, along with the rhythmic contraction (Figure 1.2) (Golenhofen 1981). The mechanism of generation of these slow waves may involve oscillations in the electrogenic Na+–Ca2+ exchange mechanism, since they are blocked by ouabain, an inhibitor of Na+, K+-ATPase which is responsible for the Na+ pump (Tomita 1981).
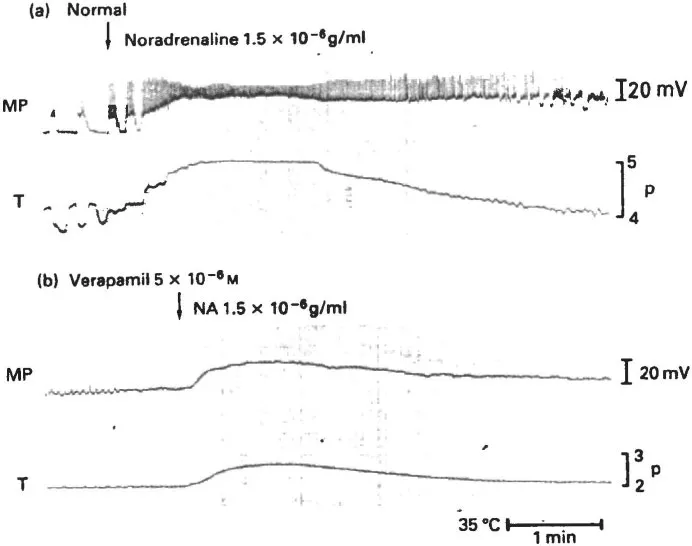
Figure 1.2 Membrane potential (MP) and tension development (T) of guinea-pig portal vein smooth muscle (a) under normal conditions and (b) in the presence of the Ca2+ channel antagonist, verapamil. Noradrenaline (NA) was added at the arrow, inducing an increase in the firing rate of spike potentials, sustained rather than slow wave depolarizations and a sustained contraction in place of phasic contractions. Verapamil blocks the slow waves. Reproduced with permission from Golenhofen et al. (1973).
The degree of spontaneous myogenic activity varies from muscle to muscle; even different blood vessels display varying amounts of myogenic activity. For example, the guinea-pig and rat portal veins show spontaneous activity whereas rabbit aorta and ear artery do not.
Addition of contractile agents, such as Ach or noradrenaline, induces an increase in firing rate of the spike potentials, a sustained continuous depolarizat...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- 1 Anatomy and physiology of the autonomic nervous system
- 2 Sympathetic neurotransmission
- 3 Adrenoceptors: classification and distribution
- 4 Sympathomimetic amines: actions and uses
- 5 Adrenoceptor antagonists
- 6 Drugs affecting storage and release from sympathetic neurones
- 7 Neurotransmission at parasympathetic nerve endings
- 8 Parasympathomimetic amines
- 9 Antagonists at muscarinic cholinergic receptors
- 10 Anticholinesterases
- 11 Drugs affecting autonomic ganglia (including the adrenal medulla)
- 12 Non-adrenergic non-cholinergic autonomic transmission
- 13 Receptors and signal transduction pathways involved in autonomic responses
- 14 Supersensitivity and desensitization
- References
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Autonomic Pharmacology by Kenneth J Broadley in PDF and/or ePUB format, as well as other popular books in Medicine & Anatomy. We have over 1.5 million books available in our catalogue for you to explore.