
eBook - ePub
Community Care in England and France
Reforms and the Improvement of Equity and Efficiency
- 228 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Community Care in England and France
Reforms and the Improvement of Equity and Efficiency
About this book
First published in 1998, the aims of this book are: the comparison of community care service and financing systems, the comparison of reform arguments and history over the last decade, the comparison of who uses how much of what services, and with what impact on their needs and the probability of having to enter institutions for long-term care. The book breaks new ground by comparing systems from a new perspective and describing contemporary reform argument and proposals for the first time in the English language. It presents new evidence from the most ambitious collection and analysis of quantative data so far made for the comparison of the two countries (based on matched area samples collecting comparable information about cohorts of new users on two or more occasions). The book also shows how the need-related circumstances of users differ between countries and within each country between areas. The book shows how and why higher levels of the French cash benefit for community care had more effect on the central policy goal than its British counterpart, how higher levels of services generally had little impact on it in either country, but on average, how the effect of the British services were much greater.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part I
1 English and French policy goals and service systems: vivent les différences
Arrangements for securing the financing and provision of services reflect the different broad models of social policy of which each is an example: often (inadequately) described as Bismarckian social insurance model supplemented with social assistance in France; the ‘Beveridgean welfare state’ model in England. Esping-Andersen (1990) described characteristics of the social insurance model as ‘conservative’ and ‘corporatist’. French commentators themselves have identified these characteristics in the French system (Henrard, 1994).
Each of a number of differences between the English and French systems can be hypothesised to affect many aspects of the efficiency of the systems.
1. Concentration of responsibility, authority and accountability
It could be expected that the greater the concentration of responsibility, authority and accountability for setting and achieving goals, the greater its efficiency. The less the concentration, it might be hypothesised, the more difficult would be coordinated policy action at all levels, reflecting the greater diffusion of power and so the greater number of conflicting goals to be reconciled;1 and the less likely would be the flexibility in the distribution and use of resources through time required for achieving important and changing goals effectively and efficiently.
The British system has inherited a high degree of concentration of authority, responsibility and accountability at every level: the political and national executive level, the local level, and the field level. In the French system, they are fragmented at all of these levels, as is commonly found in countries with variants of a Bismarckian social insurance model.
The financing system is considered to be complex and rigid (Joel and Martin, 1994). The caisses de retraite are particularly important because they have a discretionary role in financing home care of the aide ménagère (home help) type. They were separated from the assurances maladie only in 1967 (Henrard et al., 1991, p.101). The financial position of the caisses differs greatly, reflecting the fortunes of industries and occupational groups and, in particular, the ratios of beneficiaries (retired people) to contributors (in paid employment). They have had great latitude in their policies for the subsidisation of home help. Therefore, the caisses operate different policies about what level of subsidy for home care is given to whom (Curtis et al., 1992; Commissariat général du plan, 1991, p.55; Henrard, 1994).2
The structure of the system can make it difficult for the caisses to implement a targeting policy. The outcome of CNAV Circulaire No. 86/93 is an example. Issued by the national director of CNAV (Caisse nationale d’assurance vieillesse), it was intended to improve targeting of home help provision on the most dependent, by requiring each region to attain a quota whereby 6 per cent of cases would receive over 30 hours help per month. The regions were reluctant to accept this, since it was often at variance with their own targeting criteria. So also were service providers. However, in their case, this was because in many départements, the conseils généraux had a separate policy of favouring payment of the ACTP cash allowance to dependent elderly people. The effect of that was to debar the recipients from receiving intensive levels of home help, thus frustrating the service provider’s efforts to meet the CNAV 6 per cent quota.
At the regional, county and larger municipality levels, there is again diversity in responsibility, authority and accountability for financing. For example, within the framework of the régime gêneral, the assurance maladie (CNAM) has regional tiers of conseils d’administration who jealously guard their autonomy in the implementation of the national policy.
This fragmentation of financing affects supply, so working through to the level of the small area and the individual case. The criticisms include some made in the UK since the late seventies. There are many examples.
• People tend not to choose to enter homes, and do not play an active part in the processes by which they end up there: ‘il est en effet remarquable que l’initiative d’entrée en établissement échappe presque entièrement à l’intéressé’ (Attias-Donfut et al., 1994, p.20).
• Aide ménagère is not particularly targeted at those with great handicap.3
• The tasks performed are neither those which correspond to the handicaps of the recipients,4 nor the ones which make admission to institutions for long-term care most likely. For instance, they provide too little sitting for the relief of carers, and there is insufficient flexibility in the timing of interventions: it is not available out of office hours, at weekends and on bank holidays, for example.
• Instead of reforming the existing services and consolidating them into coherent structures at the local level, with the concentration of authority and responsibility and accountability for their coordination, services ‘have been piled on top of one another without any general arrangement for making them coherent’ (Guillemard and Frossard, 1993, p.256). Henrard (1994) likewise writes of a system of innovation by ‘sédimentation’.5
• Assessment practice has varied greatly. One consequence is that some progressive organisations have been attempting to make the outcomes of the assessment process more reliable by the use of standardised assessment forms and reviewing allocations as needs change (Curtis et al., 1992, p.350; Colvez et al., 1995; Puech and Colvez, 1995). Another is that there has been pressure to standardise the assessment protocols used in allocating the new benefit (‘prestation’) for long-term care for elderly people. There is the same interest in second-generation assessment-focused systems of the RAI (resident assessment instrument) type among some French research groups as there is in other countries.
However, there are problems which are different. For instance, the médecins libéraux (fee-for-service general practitioners) are an all-affecting source of distortion, particularly when associated with the high prestige and great power of the medical profession. There are more physicians in relation to the population than in England, and they compete for patients in the fee-for-service system. They therefore have an incentive not to gate-keep like the British GP.6
The consciousness of ineffectiveness and fragmentation is one reason for the French preoccupation with coordination since the Lion report of 1981 (Commissariat général du plan, 1981). The Schopflin report perceived coordination to be one of the three preconditions for efficiency/effectiveness (‘efficacité’) of the home care services (Commissariat général du plan, 1991, p.54).7,8 The logic of the demonstration projects launched by Simone Weil and supported by President Chirac combines the prestation dépendance9 with care management features: a standardised assessment protocol, a coordination around the person and family to provide the information and ‘son orientation pour leur utilisation’; and coordination of the packaging of service.
The ‘dualisme between health and social care of which the French complain exists in the UK also, save that the metaphor suggests sets of almost irreconcilable bipolarities and oppositions. And in the UK, the structural separation and cultural, procedural and institutional differences were, until recently at any rate, accompanied by a larger community care system covering a higher proportion of long-term care; one whose role is being extended by the more systematic redistribution of the community and long-term care function from health to social care. The effect is to concentrate long-term care in community social care which has itself been made more coherent.
An economically (or fiscally) efficient choice between modes of care is less likely in France. One reason is that the English concept, ‘value for money’, has not been consistently promoted by leaders of French policy opinion for the choice of care mode, despite some small studies in the late eighties and one distinguished work published in the early nineties (Bouget et al., 1990). In contrast, the economics of the costs and benefits of individual choices of alternative care models has been an important and well-published theme of the policy-analytic critiques which preceded the English reforms of the early nineties (Audit Commission, 1985, 1986; Davies and Challis, 1986; Davies et al., 1990).
A second reason is the fragmentation of the system in France. The British system has an arrangement which creates pressure for the benefits and costs to the public funders of individuals’ choice of care mode to be taken into account. For instance, authorities are increasingly encouraging care managers to take into account costs to the social services department. In contrast, although the French system has as one of its aims the support of persons at home, and its critiques comment on the excessive propensity to enter institutions, there are few arrangements to make the system efficient in that respect, or even to make the professional workers conscious of the need to do so.
2. Balance between benefits in cash and kind
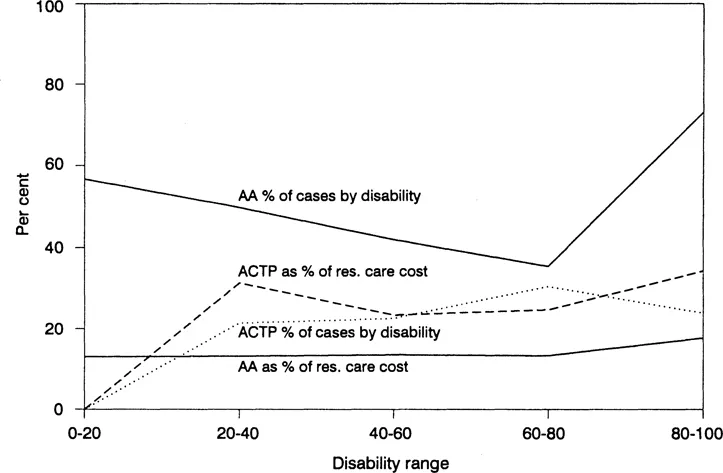
The guiding metaphor in France being insurance, the subsidy is seen as an entitlement, if claimants demonstrate the ‘insured event’. Cash benefits have played a larger part than in the UK: ‘dans le système français, il s’agit surtout de prestations en espèces ou d’aides fiscales et exonérations sociales. Les services et prestations en nature occupent une place marginale’ (Commissariat général du plan, 1991). Attendance allowance is the principal cash benefit to users for the procurement of care in the UK. The nearest French equivalent is the allocation compensatrice pour tierce personnes (ACTP).10
Since 1987, fiscal subsidies and the simplification of procedures in France have raised the incentives to use the ACTP to employ help directly. There has been continuous publicity which has raised its profile — including, most recently, widespread political justification of the benefits by their effects on generating employment. Its flexibility has been praised (Commissariat général du plan, 1991). The effect is to create competition between direct employment and the consumption of formal services.11
Figure 1 compares the English levels measured thus with the distribution in the French data. It will be seen how much higher the cash benefit can be in France in proportion to the relevant cost of residential care. However, in neither does there appear to be a clear correlation between the probability of receiving the benefits and the level of disability, save that in France the ACTP is not received by the least disabled.
3. Focus of eligibility on the person
In France, this too follows from the application of the insurance metaphor. The focus of eligibility is the individual.
However, there is considerable gerontological evidence showing how the incidence of subsidies is substantially determined by the provision of informal caregiving in most countries, irrespective of financing system. Applying eligibility and allocation criteria based solely on dependence causes either those in most need according to the judgements to obtain too little on average, or programme costs to be much increased (Davies, 1992). The argument has been particularly important in Israel and the USA (Habib and Windmiller, 1992). It i...
Table of contents
- Cover
- Title Page
- Copyright Page
- Table of Contents
- List of tables, boxes and figures
- Preface
- Introduction
- Part I
- Part II
- Part III
- Annex: Need-related circumstances, caregiver and service responses and destinational outcomes during two years: the French sites compared
- Glossary
- References
- Subject index
- Author index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Community Care in England and France by Bleddyn Davies,José Fernández in PDF and/or ePUB format, as well as other popular books in Social Sciences & Social Work. We have over 1.5 million books available in our catalogue for you to explore.