First published in 1999, this eclectic collection of papers examines quality management in health care from a variety of standpoints. Managers, health care professionals and patients all have valid – but often differing – perspectives on the nature of quality, its creation and maintenance. This book explores these perspectives, beginning by asking such fundamental questions as 'Is health care a business?', 'How should health services be designed?' and 'What is quality of care?'. Subsequent chapters then address the practicalities of measuring and improving health care quality. The chequered history of clinical audit is exposed in the UK (essentially the Plan-Do-Check-Act cycle familiar to quality improvement specialists), and lessons are drawn for managerial action needed to increase the impact of such activities. These lessons have wider relevance to all involved in promoting the principles of continuous quality improvement (CQI). In addition, exploration of the growing role of performance indicators raises important issues about their meaningfulness and instrumentality in effecting real change. Improving clinical quality is now at the top of the agenda for many health systems. This book reviews the challenges faced and the tools available to meet them. It should prove valuable to a wide range of health care stakeholders interested in broadening their understanding of this rapidly developing field.

eBook - ePub
Managing Quality
Strategic Issues in Health Care Management
- 233 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Managing Quality
Strategic Issues in Health Care Management
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
SociologyIndex
Social SciencesSECTION 1
SCENE SETTING
1 Is Health Care a Business? An Analysis of Health Care, and its Consideration as a Business
Introduction
This question is now more pertinent than ever in the UK, as the public sector component of the health care industry moves from being structured as a competitive internal market to a format based on cooperation among organizations.
The National Health Service (NHS) was structured as an internal market beginning in 1989 (Secretaries of State, 1989b). This ‘reformed’ structure resulted in:
• separation of purchasers of health care from providers;
• establishment of new organizations such as NHS trusts and GP fundholders;
• an implicit, competitive management style to compete internally for contracts.
Resources for the Conservative reforms which drove the NHS remained limited, and the idea was that the competition among providers would ensure both enhanced cost effective care, and higher quality. However, shortly after these reforms began being implemented, government ministers began to downplay the business and competitive nature of the new structure. These changed views resulted from different managerial and ministerial priorities, and, in one case, the then Minister of State for Health, William Waldegrave, signalled that the language of business had influenced the NHS too much, and that ‘the NHS is not a business, it is a public service and a great one’ (Waldegrave, 1990).
This repositioning of the NHS by the Conservatives coincided with Labour’s continuing opposition to the internal market, resulting in the publication of its NHS proposals, which focused on moving from competition to cooperation (Labour Party, 1995). Upon assuming power in 1997, the new government quickly moved to reorientate the NHS. Viewed from a Scottish perspective, particularly recognizing the distinctive nature of the NHS in Scotland (NHSiS), and its anticipated relationship to the pending Scottish Parliament, the new government quickly reaffirmed the nature of the NHS as a ‘public service’ (Galbraith, 1997). The new framework for the NHSiS was introduced through a White Paper that retained the separation of purchasers and providers, but removed the explicit competitive nature of health care provision (Secretary of State for Scotland, 1997).
However, in framing a cooperative and partnership nature to health care provision for the NHS in Scotland, the Scottish Office took firm control of health care objective setting and accountability, and therefore, implicitly, health care delivery. This was presented by indicating that the Management Executive in charge of the NHSiS would be regarded as ‘head office’, (Secretary of State for Scotland 1997), and that it viewed the ‘NHS in Scotland as a ‘firm’ to be managed, not an industry of competing businesses to be regulated’ (Scottish Office, 1997a). Through taking charge, the Management Executive, operating from St Andrew’s House in Edinburgh, will set performance indicators (financial and clinical particularly), appoint managers who can deliver its objectives, and manage proactively the whole process of health care delivery; St Andrew’s House will therefore provide a clear lead in both setting tasks and governing behaviour.
The above discussion focuses on the NHS, which is too often regarded as standing for ‘health care’ (Deffenbaugh, 1994a). In taking a step back, however, and answering the question ‘Is health care a business?’, it is essential first to address the concept of health care, leading on to an assessment of its nature as a business. The following sections present the analysis in this order.
Health Care
How health care is described depends on where one is sitting, and what is viewed through the window:
• viewed from the NHS, health care is considered to be the delivery of services to patients; while
• viewed from industry, health care is thought of as the manufacturing of products and the delivery of services ultimately to be used by patients and the wider public.
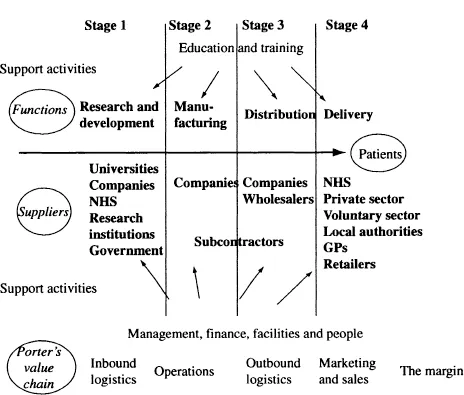
Rather than viewing health care through a window on the ground, the following discussion goes five miles up and considers the concept of health care from a strategic and holistic perspective. The vehicle for this analysis is what is called the ‘health care continuum’ (Deffenbaugh, 1994a).
The health care continuum, illustrated in Figure 1.1, represents a holistic view of health care, recognizing the impact of the following discreet, yet interlinked, stages on each other: research and development, manufacturing, distribution, and delivery. For each of these functions, there are a number of suppliers; support activities also impact on each area. The stages of the health care continuum are discussed in turn below.
Stage 1 – Research and Development
Players in the research and development (R&D) stage include companies, universities, research institutions, the NHS and government departments. R&D provides the foundation for new product development, and underpins the shape and structure through which health care will ultimately be delivered to patients. The fundamental basis for research and development is indicated by the level of expenditure in the pharmaceutical industry, which, as the Financial Times commented on the proposed SmithKline Beecham and American Home Products merger, ‘It’s the research, stupid’ (‘Lex’ column, 1998).
The fundamental importance of R&D is indicated by the level of this expenditure in the pharmaceutical and health care industries. Table 1.1 below from the UK R&D Scoreboard (DTI, 1997) presents the comparison of UK to international R&D in these industries.
Table 1.1 R&D/sales ratios (%)
Sector | UK | International |
Health care | 3.7 | 11.3 |
Pharmaceuticals | 12.0 | 12.2 |
While the UK compares favourably in spharmaceuticals, it lags dramatically in health care. The annual R&D Scoreboard, published by the UK Department of Trade and Industry (DTI) since 1991, shows that average spending on R&D by the world’s largest industrial companies (including defence and pharmaceutical companies) has remained steady at about 4.4 per cent of sales, but the UK overall is only 2.3 per cent.
The close linkage of R&D to patient care is now recognized by the NHS, resulting in the production of the Research and Development Strategy for the NHS in Scotland (Chief Scientist Office, 1993). Universities and NHS hospitals, in partnership, must now ‘earn’ research and development funds, through focusing on the outcome of R&D expenditure, which currently amounts to £38.5m in the NHSiS – £28m goes to trusts to support recurring funding, and £10m goes towards health research grants, mainly to universities. The emphasis is increasingly to translate R&D from ‘bench to bedside’, and this has been reinforced through the recent White Paper by establishing the Scottish Health Technology Assessment Centre (Secretary of State for Scotland, 1997).
A tangible example of the linkage between R&D in academia and the delivery of patient care at the bedside is the establishment of the Clinical Research Facility (CRF) in Edinburgh, with the main facility based at the city’s Western General Hospital. Supported by a £4m grant to the University of Edinburgh from the Wellcome Trust, the CRF will conduct patient-focused clinical research into a range of common diseases, including cancer, diabetes and stroke illnesses.
A further dimension of R&D is the trend towards commercialization of research and new product investigations from academia into business. The drivers within academia include the aim to attract commercial funding, but also to provide an output for R&D that is not carried out for the sole purpose of research alone. The drivers for industry are to ensure a stream of new products and processes which underpins the commercial viability of businesses.
In a macroeconomic sense, the benefits of R&D and commercialization are recognized by Scottish Enterprise through its emphasis to grow the economy via new company formation. Spin-outs from academia, often based on commercialization of R&D, will play a key part in enhancing business birth rate in Scotland (McVey, 1996).
The case can therefore be made for research and development as the first stage of the health care continuum, without which manufacturing will be constrained and uncompetitive.
Stage 2 – Manufacturing
This is the second stage of the health care continuum and results from R&D to produce a steady stream of new and creative products and processes. However, the market is very discerning, and very unforgiving of manufactured products that do not meet customer requirements, so the link must therefore be very strong from R&D through manufacturing to ultimate consumption. This is nothing new – as Adam Smith indicated, ‘consumption is the sole and purpose of production’ (Smith, 1776).
The health care manufacturing sector comprises companies in a number of fields: pharmaceutical, biomedical, bioengineering, medical equipment, biotechnology, disposables, etc. These manufacturers, largely in the private sector in the UK, will in some cases manufacture end products themselves, or form part of a supply chain process resulting in end product manufacturing. Across the UK, the profile of companies (Dun & Bradstreet, 1998) is towards the small and medium-sized enterprise (SME) end of the spectrum – sales of less than £15m – as illustrated in Table 1.2.
Table 1.2 Manufacturing companies in the UK
Sales (£) | No. | % |
< 15m | 25,864 | 88.6 |
15m–30m | 1,566 | 5.4 |
30m–60m | 836 | 2.9 |
60m–90m | 305 | 1.0 |
>90m | 605 | 2.1 |
Total | 29,176 | 100.0 |
Within Scotland, the manufacturing sector overall accounts for 7.5 per cent of VAT-based enterprises, while for England the figure is 9.9 per cent (Office for National Statistics, 1996). Health industry enterprises account for only .53 per cent of the overall businesses in Scotland, and .57 per cent in England. The manufacturing and health care sectors in Scotland are underdeveloped, which reinforces the strong business relationship among not only various parts of the UK, but also within Europe and worldwide.
It is not only products which are ‘manufactured’, but also services, and these are also included in Stage 2 of the health care continuum. The financial and business services sector alone accounts for 20 per cent of Scottish gross domestic product, compared to 18 per cent for manufacturing (Scottish Office, 1997b). The availability and extent of services equally provides an outlet for R&D, such as with computer information systems and manufacturing processes.
A further dimension to manufacturing, linking this stage of the continuum to support activities, is the ‘manufacturing’ of specialist skills embodied in the ro...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- List of Figures
- List of Tables
- Acknowledgments
- Preface
- Section 1: Scene Setting
- Section 2: Quality in Health Care
- Section 3: Using Performance Indicators
- List of Contributors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Managing Quality by H.T.O . Davies,M. Tavakoli,M. Malek,A. Neilson in PDF and/or ePUB format, as well as other popular books in Social Sciences & Sociology. We have over 1.5 million books available in our catalogue for you to explore.