![]()
1 & 2: Questions
1 A 6-year-old cat presents with progressively stertorous respiratory sounds, periods of open-mouth breathing at rest, and reduced exercise tolerance. There is no history of sneezing or coughing and no external nasal discharge. Airflow is absent from both external nares. Flexible endoscopic examination of the retropharynx reveals an obstructing soft tissue mass occluding both choanae (Figure 1.1). The obstructing tissue is smooth and light pink in color.
FIGURE 1.1
i. What is your clinical diagnosis? What other differential diagnoses should you consider for a mass in this region?
ii. What, if any, additional diagnostic imaging would you recommend in this case? Why?
iii. What treatment options are available for nasopharyngeal polyps?
2 A client presents with a mixed breed dog that has chronic, mixed, small and large intestinal diarrhea. The client is convinced that their dog has a gluten sensitivity and tells you that “everyone knows that dogs can get celiac disease.”
i. Gluten-sensitive enteropathy has been conclusively diagnosed in which dog breed(s)?
ii. Which protein(s) do patients with gluten-sensitive enteropathy react to?
iii. Your client is determined that their dog should switch to a gluten-free diet, before any other diagnostic steps. How would you respond?
1 & 2: Answers
1 i. The history, clinical signs, and endoscopic imaging results are most consistent with the presence of an inflammatory polyp occupying the retropharynx and choanae. Differential diagnoses that should be considered in this region include nasal lymphoma, carcinoma/adenocarcinoma, and granuloma formation.
ii. Nasopharyngeal polyps arise from either the Eustachian tubes or middle ear, secondary to chronic inflammation. It is important to assess the middle ears for evidence of disease (otitis media), as this can influence both therapeutic planning and the prognosis for recurrence. Plain radiography can be utilized, but there is the potential for a false negative diagnosis. In some studies, plain radiography has a false negative rate of 25% in cats with otitis media. Advanced imaging, either computed tomography or magnetic resonance imaging, are very useful in assessing the middle ears and status of the osseous bulla. The presence of severe bulla disease argues for bulla osteomy surgery.
iii. If accessible, particularly when the polyp is visible within the caudal oral cavity with retraction of the soft palate, manual distraction of the polyp may be attempted. In the case shown here, the polypoid tissue was not accessible for manual extraction and surgical resection along with bulla osteotomy was carried out.
2 i. Gluten-sensitive enteropathy was definitively diagnosed in the Irish Setter in the United Kingdom in the late part of the 20th century (Figure 2.1). The condition had an autosomal recessive mode of inheritance in these dogs. While conclusive diagnosis of gluten-sensitive enteropathy in dogs is now rare, it is reasonable to expect that some individual dogs may present with gluten-responsive gastrointestinal disease. At the time of writing, there is growing controversy in the human medical literature regarding “non-celiac gluten sensitivity,” an umbrella term for gastrointestinal symptoms that show response to gluten avoidance yet have not met the typical diagnostic criteria for celiac disease or wheat allergies in human patients.
FIGURE 2.1
ii. The major protein(s) leading to gastrointestinal inflammation in patients with gluten-sensitive enteropathies are the gliadins. Ideally, this disease is diagnosed by documenting resolution of clinical signs on a strict gluten-free diet followed by return of clinical signs after an oral gluten challenge. The Irish Setter cases were diagnosed in this manner, leading to a firm diagnosis of gluten-sensitive enteropathy.
iii. As long as the new diet is appropriately nutritionally balanced and appropriate for the dog’s age and breed, there is no real argument against making this diet change. However, while gluten sensitivity certainly has been well documented in a select group of dogs (the Irish Setters), this does not mean that other diagnostic investigations such as parasitology, assessment of water-soluble vitamins, and diet modification trials with new protein sources can be neglected. Combining diet trials with a gluten-free formulation and a novel protein source would be an ideal way to acknowledge the client’s concern and if successful would support the diagnosis of food-responsive enteropathy in this patient.
![]()
3 & 4: Questions
FIGURE 3.1
FIGURE 3.2
3 A 1-year-old male Pug was presented with a 2-month history of inappetence and mild diarrhea. The appetite is reported to wax and wane. The patient has been tempted with a number of different novel protein diets. The diarrhea is characterized as small intestinal. The patient has not responded to courses of metronidazole, fenbendazole, and symptomatic administration of maropitant. The patient is currently on recommended vaccinations and receives routine heartworm and external parasite prophylaxis.
On physical examination, the dog has a normal body temperature (38.6°C, 101.5°F) and weighs 5 kg (11.0 lb) with a 2/9 body condition score. There was generalized muscle wasting, but otherwise the physical examination was unremarkable.
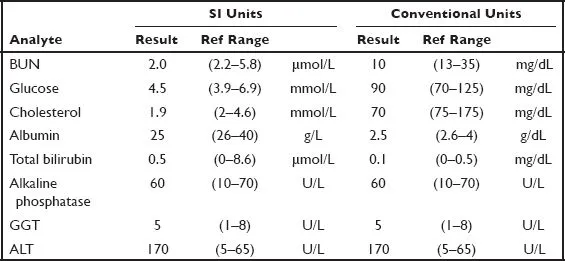
Preliminary diagnostic evaluation demonstrates a mild increase in alanine aminotransferase activity (2× upper limit of normal) and a mild decrease in serum albumin and cholesterol. Other pertinent clinical chemistry results are provided below.
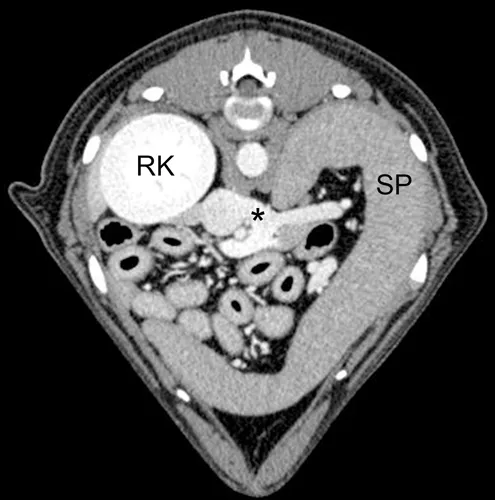
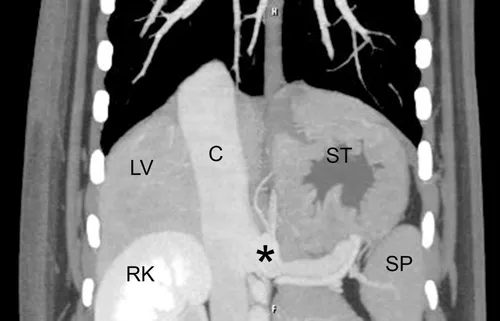
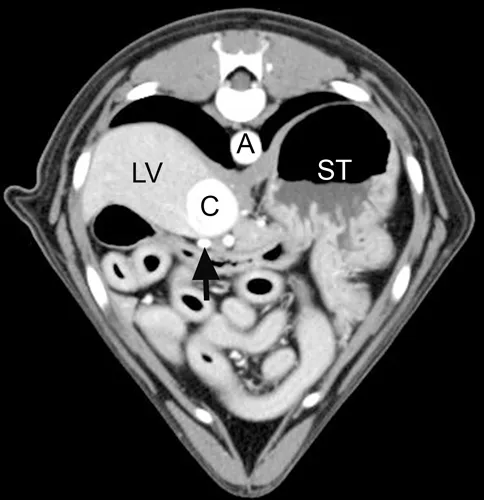
A CT angiographic study of the portal venous system was performed. Transverse and dorsal plane images are presented (Figures 3.1–3.3). A portosystemic shunt (asterisk, Figures 3.1 and 3.2) arises from the splenic vein and terminates in the caudal vena cava (C) from the left side, just cranial to the celiac artery. Cranial to the insertion of the shunting vessel, the caudal vena cava is widened. Cranial to the insertion of the splenic vein, the portal vein abruptly narrows (arrow, Figure 3.3). The liver is small and only very small portal branches are seen entering hepatic parenchyma (not shown). The patient has a few small mineral cystoliths (not shown). RK = right kidney, ST = stomach, SP = spleen, LV = liver, A = aorta.
FIGURE 3.3
i. What is your interpretation of the imaging findings?
ii. What is the most likely diagnosis?
iii. What additional diagnostic testing could be used to confirm your diagnosis?
iv. How would you approach the management of this case?
v. What is the likely prognosis?
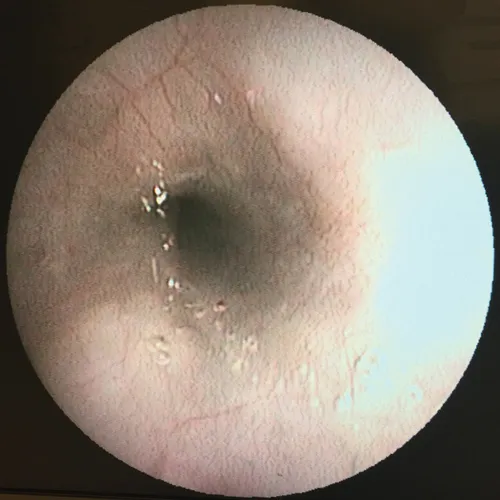
4 A 9-year-old spayed female cat presents with a history of progressive stertor. Figure 4.1 shows the caudal nasopharynx as visualized by flexible endoscopy.
FIGURE 4.1
i. What is your clinical diagnosis?
ii. How does this lesion arise?
iii. What treatment options are available?
3 & 4: Answers
3 i. The patient has a single, extrahepatic portosystemic shunt with secondary microhepatia and cystolithiasis. The splenocaval morphology of the shunting vessel is one of the most common types.
ii. Extrahepatic portosystemic shunt.
iii. Computed tomographic study, bile acids, ammonia tolerance test, scintigraphy.
iv. Medical management (anti-epileptic drug therapy, lactulose, restricted protein diet, and antimicrobial therapy) followed by surgical attenuation of the shunting vessel is recommended. Protein restriction sufficient to ameliorate clinical signs is often attainable with moderate protein restriction (i.e., prescription renal diet, geriatric diets) and is recommended over severe protein restriction in hepatic diets if possible in juvenile patients.
v. The prognosis ...