Pulsed Electromagnetic Fields for Clinical Applications presents the historical development, the state of art, and the future of the application of pulsed electromagnetic fields (PEMFs) for the treatment of various medical problems, including initiating various healing processes from delayed fractures and pain relief to multiple sclerosis and Parkinson's disease. The emphasis is on the development of scientific methods to be implemented in clinical application.
In perspective, this modality provides a practical, exogenous method for inducing cell and tissue modification attempted to the injured tissues to their normal physiological status. The book reviews the current state of equipment for PEMFs and highlights worldwide therapeutic achievements.
It explores the past, present, and future of PEMF therapies.
It presents the development of theory and laboratory research during the last 70 years.
It reviews the available equipment for PEMF.
It reviews the state of the art of worldwide therapeutic achievements.
It includes recent achievements and applications of electroporation modalities.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Electromagnetic field (EMF) therapy has a long history and is still not widely popular among medical practitioners. James T. Ryaby, Erik Waldorf, and I had decided to integrate efforts of clinicians, engineers, and scientists in presenting the state of the art in international settings. This chapter will be a brief overview of the history and state of the art of EMF therapy and will include nearly the entire spectrum of frequency ranges, starting with static magnetic field and reaching terahertz signals.
I would like to start with a brief history. Very little known is the fact that contemporary magnetotherapy begun immediately after World War II by introducing both magnetic and EMFs, generated by various waveshapes of the supplied currents. It started in Japan and quickly moved to Europe, first in Romania and the former Soviet Union. During the period 1960–1985, nearly all European countries designed and manufactured their own magnetotherapeutic systems. Indeed, the first contemporary book on magnetotherapy was published in Bulgaria by Todorov (1982).
In the USA, the first approved signal was for treatment of nonunion fractures by employing a very specific biphasic low-frequency signal (Bassett et al., 1974, 1977). A decade later, the Food and drug administration (FDA) in the USA allowed the use of pulsed radio frequency (PRF) EMF for treatment of pain and edema in superficial soft tissues.
The worldwide physics, engineering, biology, and clinical applications of various modifications of EMFs for treatment of medical problems ranging from bone unification, to wound healing, to pain control has been the subject of several books (Polk and Postow, 1986; Rosch and Markov, 2004; Barnes and Greenebaum, 2007; Lin, 2011; Markov, 2015; Barnes and Greenebaum, 2019). In these and many papers in peer-reviewed journals was published a detailed explanation of the basic science and clinical evidence that time-varying magnetic fields can modulate molecular, cellular, and tissue function in a physiologically and clinically significant manner.
Therapy using EMF developed in various stages and involved any new discovery in the basic science, especially biophysics and bioelectrochemistry. I had the privilege to be involved in some stages in this development. In the early 1980s, I was in communication with members of the Bioelectrochemical Society, attended the meetings of this society in Europe, and organized two international conferences titled “Electromagnetic Fields and Biomembranes” in my “little” Bulgaria in the second half of the 1980s. In this society, electroporation was developed as a plausible method in biophysics and later suggested as a possible therapeutic method.
The fundamental questions for engineers, scientists, and clinicians is to identify the biochemical and biophysical conditions under which EMF signals could be recognized by cells in order to modulate cell and tissue functioning. It is also important for the scientific and medical communities to recognize that different EMFs applied to different tissues could cause different effects. What “different EMFs” means is at the same time difficult and easy to define. It is easy because a signal is new if it has at least one parameter different from the previous one. The difficulties arise because very few manufacturers, distributors, or authors of a published study exactly describe the parameters of the device.
NECESSARY STEPS
Especially since the beginning of this century and the development of the Internet, a large number of devices could be found in the market. In most cases, these devices are distributed without a proper engineering and physics description. Let me point out that the ideal situation in clinical use of this technology requires the following steps:
medical diagnostics of the specific problem and desired EMF
engineering of the appropriate devices
physics/biophysics of dosimetry and selection of the device
medical therapeutics.
The first part of the equation, medical diagnostics, should identify the exact target and the “dose” of EMF that the target needs to receive. Then, physicists and engineers should design the exposure system in such a way that the target tissue receives the required magnetic flux density. Any new device must be properly characterized by physical dosimetry. Once the appropriate signal is engineered, serious attention must be paid to the biophysical dosimetry capable of predicting the EMF signals that could be bioeffective and in monitoring device efficiency. This raises the question of using theoretical models and biophysical dosimetry in selection of the appropriate signals and in engineering and clinical application of new EMF therapeutic devices.
Unfortunately, in most cases, the chain starts with the question “what signal is available?” Then the clinician applies common sense and his/her experience and intuition in selecting the protocol of treatment. Dosimetry and analysis of the signal often remains out of consideration. For this reason, many laboratory and clinical studies cannot be replicated.
PHYSICAL DOSIMETRY AND BIOPHYSICAL DOSIMETRY
We introduce here two dosimetry terms, “physical dosimetry” and “biophysical dosimetry”, because it appears that the issue of dosimetry is not properly interpreted in both the scientific and clinical communities. Physical dosimetry relates to characterization of the device with respect to engineering and physical parameters, including signal parameters such as frequency, signal shape, amplitude, repetition rate, rising time, etc. It should be pointed out that these are characteristics of the device and not the actual field distribution inside the target tissue.
Biophysical dosimetry characterizes the “dose” received by the target tissue. I suggest that the only valuable information for a clinician is that which explains the field values at the target site. This goal is easy to achieve because the magnetic properties of air and biological tissue, especially for low-frequency fields, are almost the same.
Another important issue is the fact that any physical body attenuates the electric field component and allows only the magnetic component to penetrate deep into the body. Therefore, biophysical dosimetry is mainly dosimetry of the magnetic fields. It should also be taken into account that any time-varying magnetic field induces an electric field, which in some cases might be of importance in analyzation and interpretation of the observed effects. As it was pointed out earlier (Markov, 2002, 2009), the induced electric field generates “back” magnetic fields, and this fact should be taken into account in any measurements, especially in measuring high-frequency signals.
The pulsed electromagnetic field (PEMF) signals in clinical use have a variety of designs, which in most cases are selected without any motivation for the choice of the particular waveform, field amplitude, or other physical parameters.
It is reasonable that the first and widely used waveshape is the sine wave with a frequency of 60 Hz in North America and 50 Hz in the rest of the world. From symmetrical sine waves, engineers moved to an asymmetrical waveform by means of rectification. These types of signals basically flip-flop the negative part of the sine wave into positive, thereby creating a pulsating sine wave. Textbooks usually show the rectified signal as a set of ideal semi-sine waves. However, due to the impedance of any particular design, such an ideal waveshape is impossible to achieve. As a result, the ideal form is distorted, and a short DC-type component appears between two consecutive semi-sine waves.
In addition to sine-wave-type signals, a set of therapeutic devices which utilize unipolar or bipolar rectangular signals are available in the market. Probably for those signals, the most important is to know that, due to the electrical characteristics (mostly the impedance) of the unit, these signals could never be rectangular. There should be a short delay both in raising the signal up and in its decay to zero; thereby the rectangular signal is basically trapezoid. The rise time of such a signal could be of extreme importance because the large value of dB/dt could induce significant electric current into the target tissue. Some authors consider that neither frequency, nor the amplitude is so important for the biological response but the dB/dt rate is the factor responsible for observed beneficial effects. Kotnik and Miklavcic (2006) suggested that the rectangular signals should be replaced by more realistic trapezoid signals. It appears easy to say, but it is nearly impossible technologically to generate trapezoid signals.
As the signal choice in any particular device, in most cases, is not a function of medical and biophysical criteria, especially with free Internet offering, one may find large variation in signals. Unfortunately, manufacturers and distributors have one only goal – to make money, in most cases at free press variety of claims could be found.
Which are the signals that could be the most effective and at what conditions? Are certain signal parameters better than others? It should be pointed out that many EMF signals used in research and as therapeutic modalities have been chosen in some arbitrary manner. Very few studies assessed the biological and clinical effectiveness of different signals by comparing the physical/biophysical dosimetry and biological/clinical outcomes.
It was nearly half a century since the concept of “biological windows” was introduced. Interestingly enough, three groups located in different countries and unknown to one another published almost similar papers in which it was stated that during evolution, Mother Nature created preferable levels of recognition of the signals from exogenous magnetic fields. The “biological windows” could be identified by amplitudes and frequencies and their combinations (Adey, 1993; Markov, 1994). The research in this direction requires assessment of the response in a range of amplitudes and frequencies. It has been shown that at least three amplitude windows exist: at 5–10 Gauss, 150–200 Gauss, and 450–500 Gauss (Markov, 2005). Using cell-free myosin phosphorylation to study a variety of signals, Markov’s group has shown that the biological response depends strongly on the parameters of applied signal, confirming the validity of the last two “windows”.
The first clinical signal approved by FDA for treatment of nonunions or delayed fractures (Bassett et al., 1974, 1977) exploited the pulse-burst approach. Having a repetition rate of 15 burst/s, the clinical use of this asymmetrical signal (with a long positive and very short negative component) has been very successful in healing nonunion bones for more than 30 years. The engineers assume that the cell/tissue would ignore the short negative part of the pulse and would respond only to the envelope of the burst which has a duration of 5 μs, enough to induce sufficient amplitude in the kHz frequency range. A series of modalities generate signals that consist of single narrow pulses separated by long “signal-off” intervals. This approach allows modification of not only the amplitude of the signal but also the duty cycle (time on/time off).
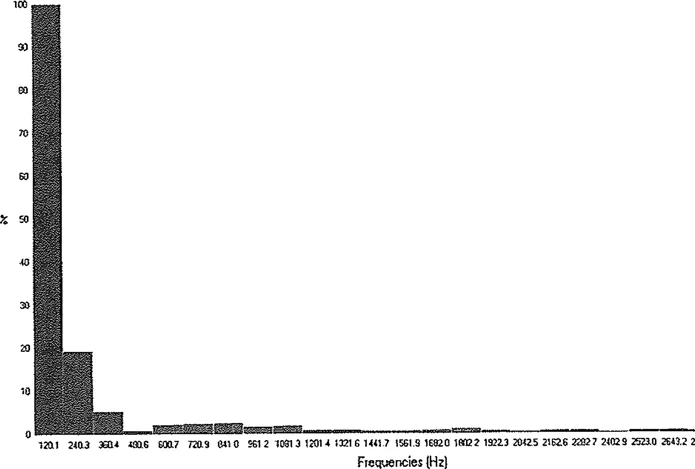
Let me point to another problem with time-varying EMF. We performed the Fourier analysis for a rectified semi-sine wave signal implemented in the therapeutic system THERAMAGTM. The spectrum shows that, at basic frequency of 120 pulses per second (pps), the first harmonic (240.3 pps) has an amplitude equal to 20% of the amplitude of the basic frequency. The third harmonic (360.4 pps) has an amplitude equal to 5% of the basic amplitude. In addition, the first 20 harmonics, up to 2,643 pps, were identified by the Fourier analysis (Figure 1.1).
FIGURE 1.1 Spectrum of harmonics at the rectified 60 Hz signal.
The importance of the impedance of the waveshape and harmonics in physics and biology remains to be determined. As for many other signals, the biophysical analysis of the rectified signal implemented in this type of therapeutic unit is practically absent. More research is needed to further clarify the importance of impedance of the system in generating and delivering appropriate signals (and their frequency components for treatment of the desired target). What does all this mean? It means that, at leas...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Table of Contents
Editors
List of Contributors
Chapter 1 Electric and Electromagnetic Stimulation: Electroporation
Chapter 2 Pulsed Electromagnetic Fields: From Signaling to Healing
Chapter 3 Biophysical Stimulation of Bone Growth in Fractures
Chapter 4 Biophysical Stimulation of Articular Cartilage for Chondroprotection and Chondroregeneration
Chapter 5 Electromagnetic Field Effects on Soft Tissues – Muscles and Tendons
Chapter 6 Clinical Use of Pulsed Electromagnetic Fields (PEMFs)
Chapter 7 Electromagnetic Fields in Relation to Cardiac and Vascular Function
Chapter 8 Toward ELF Magnetic Fields for the Treatment of Cancer
Chapter 9 Terahertz Electromagnetic Fields in Diagnostic and Therapeutic Settings – Potentials and Challenges
Chapter 10 Nanopulse Stimulation Therapy: A Novel, Nonthermal Method for Clearing Skin Lesions
Chapter 11 Calcium Electroporation – A Novel Treatment to Overcome Cancer-Mediated Immune Suppression
Chapter 12 A History of Pulsed Electromagnetic Fields
Chapter 13 A Brief History of Orthofix Medical Inc.’s Biostimulation
Chapter 14 History of the Frank Reidy Research Center for Bioelectrics
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Pulsed Electromagnetic Fields for Clinical Applications by Marko Markov, James Ryaby, Eric I. Waldorff, Marko Markov,James Ryaby,Eric I. Waldorff in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Theory, Practice & Reference. We have over 1.5 million books available in our catalogue for you to explore.