Psychotherapy and Aphasia: Interventions for Emotional Wellbeing and Relationships is an exciting international collaboration among clinical neuropsychologists, speech and language therapists and family therapists that details a range of innovative psychotherapeutic interventions to enable people with communication disorders and their families to access meaningful support.
People with aphasia and other acquired communication disorders can face significant challenges accessing emotional support. Many traditional forms of psychotherapy are based on spoken language, rendering it inaccessible for many people with communication disorders. But the book details a range of techniques that move away from reliance on spoken language, including total communication strategies, the use of meaningful objects, experiential process, group experience and mind-body practices.
Featuring clinical examples which cover a range of stroke and neurology service contexts, the book includes contributions from a range of therapeutic models; from speech and language therapy and family therapy to clinical neuropsychology, cognitive-behavioural, systemic, narrative and mind-body traditions. It therefore provides clinicians with a wide-range of practical and theoretical tools to explore when supporting survivors who experience psychological distress during rehabilitation. It is the only book aimed at both speech and language therapists and psychotherapists, and will open up new pathways to support.
A call for the speech pathology1profession to utilise stepped psychological care for people with aphasia post stroke
Brooke Ryan2,7, Linda Worrall2,7, Jasvinder Sekhon3,7, Caroline Baker3,7, Marcella Carragher3,7, Jaycie Bohan2, Emma Power4,7, Miranda Rose3,7, Nina Simmons-Mackie5, Leanne Togher4,7, Ian Kneebone6,7
Introduction
Stroke often results in significant psychological upheaval and strain (Brumfitt, 1993; Gainotti, 1997; LaFond, 1993; Lincoln, Kneebone, Macniven, & Morris, 2012; Lincoln & Kneebone, 2012; Robinson, 2010; Tanner, 2003; Thomas & Lincoln, 2006). Lincoln and Kneebone (2012) report on the prevalence and variety of psychological conditions after stroke, including depression (30%), involuntary emotional expression disorder (20%-30%), post-traumatic stress reaction (27%), apathy (22%-28%), generalised anxiety disorder (10%-30%), catastrophic reaction (20%), fear of falling (60%), and anger (17%-35%). The prevalence of psychological conditions among people with stroke is likely to continue to increase alongside Australia’s increasing ageing population and accompanied increased incidence of stroke. More than 420,000 Australian stroke survivors currently live in the community, and this is set to increase to approximately 700,000 by 2032 (Deloitte Access Economics, 2013).
Concurrent with these distressing psychological outcomes, a stroke may result in a range of physical and communication sequelae. One of the most common communication difficulties is aphasia, which is a language impairment that can affect reading, writing, talking and understanding and limits everyday conversations (Hallowell & Chapey, 2008). Approximately 30 per cent of stroke survivors have aphasia, and, whilst substantial language recovery is possible, many people will live with aphasia for the rest of their lives (Flowers et al., 2016). Aphasia appears to be a risk factor for poor mental health (Kutlubaev & Hackett, 2014; Menlove et al., 2015). Up to 70 per cent of individuals with stroke and aphasia have depression (Kauhanen et al., 2000), and up to 44 per cent have anxiety (Morris, Eccles, Ryan, & Kneebone, 2017). People with post-stroke aphasia also often report other psychological impacts, including changes in identity and sense of self, feelings of frustration and/or isolation, negative self-esteem, reduced coping abilities, stress, distress, reduced optimism and hope, changed life satisfaction and wellbeing (Brumfitt, 2006; Cruice, Hill, Worrall, & Hickson, 2010; Hilari, Needle, & Harrison, 2012; Parr, 2001; Shadden, Hagstrom, & Koski, 2008).
The communication disability imposed by aphasia influences psychological wellbeing and restricts participation in activities of choice (Cruice, Worrall, Hickson, & Murison, 2003; Hackett, Anderson, House, & Halteh, 2008; Hilari & Byng, 2009; Hilari, Wiggins, Roy, Byng, & Smith, 2003). This has a spiralling effect, with resultant poor psychological wellbeing in turn reducing frequency and enjoyment of activities and participation in previously enjoyed life roles, and interfering with adjustment and participation in rehabilitation (Brown, Worrall, Davidson, & Howe, 2010; Carota, Staub, & Bogousslavsky, 2002; Code & Herrmann, 2003; Cruice, Worrall, & Hickson, 2011; Fucetola et al., 2006). It is not surprising that one recent study found that in the first 12 months post stroke, low mood was consistently and negatively associated with successfully living with aphasia (Worrall, Hudson, Khan, Ryan, & Simmons-Mackie, 2017). Another reason why this population is particularly at risk of poor mental health is that aphasia after stroke is associated with greater disability, increased reliance on rehabilitation services and increased likelihood of being discharged to a care setting rather than home from hospital (Flowers et al., 2016).
There is a significant gap between clinical need and service provision to support psychological health in people with aphasia. The Stroke Foundation in Australia has consistently identified that access to mental health services post stroke is extremely limited (Stroke Foundation, 2018). Their latest audit found that 50% of patients had some degree of mood impairment post stroke yet one third of services reported no access to clinical or neuropsychologists in stroke rehabilitation (Stroke Foundation, 2018). These figures relate to the general stroke population, and therefore the level of psychological services provided to people with aphasia are likely to be much lower given the challenges of psychological service provision to individuals with communication disability (Ryan, Bohan, & Kneebone, 2019). People with aphasia are therefore vulnerable to poor mental health that will likely deteriorate over time because of insufficient access to treatment and support.
Mental health studies typically exclude people with aphasia because the research procedures, outcome measures or treatments are determined to be inaccessible to them (Campbell, Skidmore, Whyte, & Matthews, 2015; Townend, Brady, & McLaughlan, 2007). The impact of this exclusion perpetuates the disparity in stroke care for people with aphasia. Brady, Fredrick, and Williams (2013) described this phenomenon as “an unacceptable stroke-specific variation of the ‘inverse care law’ where people with the highest needs have the poorest evidence base and receive the least research attention” (p. 193). This lack of evidence in mental health research may also promote the false notion that people with aphasia cannot engage in any kind of psychotherapeutic or mental health–focussed intervention, largely on account of communication barriers (Dalemans, Wade, van den Heuvel, & de Witte, 2009).
Speech pathologists may be well placed to facilitate access to mental health services in people with aphasia after stroke. They have expertise in providing communication support and have a comprehensive understanding of the pervasive impact of aphasia. Speech pathologists often take on the role of “communication broker” between a person with aphasia and the stroke team. Unfortunately, a lack of formal psychological therapy training means speech pathologists may feel either limited in terms of scope of practice to deliver mental health supports/interventions or under-skilled to do so (Sekhon, Douglas, & Rose, 2015). Approximately 45 per cent of speech pathologists do not formally screen for mental health issues in their patients with aphasia and two thirds do not address wellbeing as part of their management (Sekhon et al., 2015). Whilst some people with stroke do have access to mental health practitioners, these practitioners often do not have the necessary skills to serve this group (Northcott, Simpson, Moss, Ahmed, & Hilari, 2016).
The answer to the limited psychological training speech pathologists receive may seem obvious: that speech pathologists train mental health practitioners to work with people with aphasia and/or speech pathologists co-work with mental health professionals to provide services. Whilst this model of delivery will work in some health settings, in others, integrated stroke and mental healthcare pathways do not exist, and there is potential for people with aphasia post stroke to be seen by a number of services in isolation. In practice, only one third of speech pathologists working with people with aphasia report that they frequently train mental health professionals in supportive communication strategies (Sekhon et al., 2015). Further, not all multidisciplinary stroke teams have access to a mental health professional, and specific availability of psychology services is restricted (National Stroke Foundation, 2012). On this account, people with aphasia and mental health problems are at high risk of falling through the cracks. Therefore, there is a strong and urgent need for speech pathologists to engage in this area of clinical need. The principal way this might be achieved is to embed a model within speech pathology practice by which everyone with aphasia accesses the level of support they require. For example, the most recent stroke clinical guidelines in the United Kingdom recommend that psychological care provided by stroke services be based upon three main models of service delivery (collaborative care, matched care and stepped care; Intercollegiate Stroke Working Party, 2016). The model that this article explores further is that of “stepped psychological care” (Kneebone, 2016).
Stepped psychological care
Stepped psychological care after stroke is described as the hierarchical delivery of routine assessment and interventions for emotional difficulties and psychological problems (Kneebone, 2016). This model has been demonstrated to be effective in a range of contexts with varying populations (Firth, Barkham, & Kellett, 2015) and has been applied internationally into various health services (e.g., Australian Department of Health; The National Health Service of Great Britain and Northern Ireland). Stepped psychological care models are based on increasing levels of tailored intervention and have usually been described to either have three or four levels progressing from “low” intensity to “high” intensity interventions (e.g., National Institute for Health and Clinical Excellence, 2009; National Institute for Health and Clinical Excellence, 2011; Kneebone, 2016).
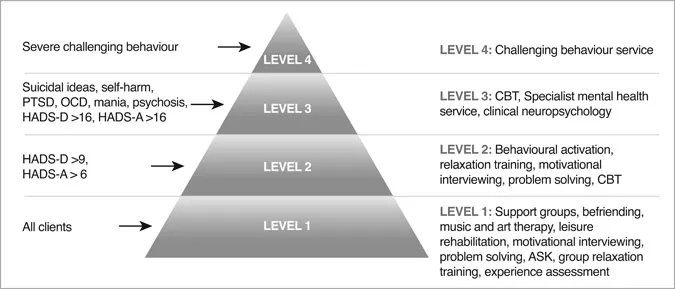
Within the literature, descriptions of stepped psychological care and the level of intervention a person typically first receives vary (Intercollegiate Stroke Working Party, 2016). Kneebone (2016) has provided a narrative review and proposed a model for stepped psychological care after stroke (Figure 1.1). In Kneebone’s (2016) stepped psychological care approach, four levels of intervention are described, and a person is matched to the intervention level that most suits their current need. In other words, an individual does not generally have to start at the lowest, least intensive level of intervention to progress to the next “step”. Rather, they enter the system and have their service level aligned to their requirements. If at any point their condition deteriorates or if they do not respond to the intervention, they proceed to the next step in the model where the service becomes increasingly tailored and is delivered by more specialised practitioners. Similarly, someone who has benefitted from a higher-level intervention initially might “step down” and maintain their treatment outcome with a less-intensive intervention.
Figure 1.1 A revised model for stepped psychological care after stroke
Note: ASK = Action Success Knowledge Program for People with Aphasia, HADS = Hospital Anxiety and Depression Scale, -D Depression subscale, -A Anxiety subscale, CBT = Cognitive Behavioural Therapy, PTSD = Post Traumatic Stress Disorder, OCD = Obsessive Compulsive Disorder.
Source: Reproduced with permission from Kneebone, 2016
In Kneebone’s (2016) stepped psychological care model, level 1 intervention, or the “lowest” intensity intervention, is described as appropriate for all stroke survivors because of the psychological impact of stroke. At this level the therapeutic target is prevention of the onset of mental disorders and treatment of “sub-threshold problems” such as general difficulties with coping and experience of general distress. Level 2 interventions target mild/moderate symptoms of impaired mood. Levels 3 and 4 of the model are for severe and persistent disorders and/or challenging behaviours (Kneebone, 20...
Table of contents
Cover
Half Title
Series Page
Title
Copyright
Contents
Editors’ foreword
1 Time to step up: a call for the speech pathology profession to utilise stepped psychological care for people with aphasia post stroke
2 The importance of syntax in making meaning and emotional adjustment: a brief psychodynamically oriented intervention in receptive aphasia
3 A personal construct psychology approach to aphasia
4 Supporting families with aphasia to explore relationships
5 A preliminary study of “Laboratorio di Conversazione Narrativa”: group psychotherapy supporting communication for people with aphasia
6 Structured narrative therapy for children with acquired brain injury and severe communication difficulties
7 Mindfulness interventions for people with aphasia – case evidence from individual and group therapy formats
8 The potential contribution of mind-body interventions within psychological support following aphasia: a conceptual review and case study
Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Psychotherapy and Aphasia by Kate H. Meredith, Giles N. Yeates, Kate Meredith,Giles Yeates,Kate H. Meredith,Giles N. Yeates in PDF and/or ePUB format, as well as other popular books in Psychology & Audiology & Speech Pathology. We have over 1.5 million books available in our catalogue for you to explore.