If we will ever achieve Paul Ehrlich's "magic bullet," that is, a molecule which goes with high selectivity to the therapeutic target site, does what it needs to do, and is subsequently cleared from the body, the practice of safety assessment will have to change. Nonclinical Drug Administration: Formulations, Routes and Regimens for Solving Drug Delivery Problems in Animal Model Systems seeks to address a trio of objectives that, though separate, are linked and central to biomedical science and, ultimately, medicine. Rather seeing these as separate "silos," those working in nonclinical safety assessment will have to view these three in an integrated manner and to regularly and thoughtfully incorporate new information and technology.
The trio of objectives this book explores are: first, to present how to deliver more of a drug product systemically to facilitate the regulatory need for evaluating safety and efficacy in animal species (at elevated exposure levels) prior to advancing the drug to human testing; second is to achieve better tolerance to therapeutics administration in test animals and humans which achieves objectives 1 and 3; and third, to explore ways to improve on therapeutic target receptor delivery performance, therefore improving both clinical pharmacodynamics bioavailability and specificity.
The book's ten chapters assemble the basic concepts, principles and hypotheses involved in quantitative receptor and chronological organism interaction dynamics central to the successful development of new therapeutics which depend on systemic administration to achieve desired therapeutic goals and in so doing avoid outcomes which limit, marginalize, or preclude the therapeutic use of so many molecules.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
This book seeks to address a trio of objectives that, though separate, are linked and central to biomedical science and, ultimately, medicine. For nonclinical safety assessment, failure to view these three in an integrated manner (rather than the current practice as separate “silos”) and to regularly and thoughtfully incorporate new information and technology has largely frozen in time, for decades, the practice of safety assessment.
The first objective is to present how to deliver more of a drug product systemically to facilitate the regulatory need for evaluating safety and efficacy in animal species (at elevated exposure levels) prior to advancing the drug to human testing, with the goal of translating the same lessons into humans and optimizing clinical use.
The second objective is to achieve better tolerance of therapeutics administration in test animals and humans which achieves the first and third objectives. Tolerance should be either local (at the site or organ of administration) or systemic (across the entire organism, especially at distal “off target” sites). Local tolerance is usually determined by evaluating either inflammation (erythema and edema) and tissue histopathology signs at the site of intravenous administration or changes in measures of the formed cell elements in the blood. Determining systemic tolerance (general toxicology) is most often what is entailed in general (or “systems”) toxicology (Gad, 2016).
The third objective is to explore ways to improve therapeutic target receptor delivery performance, therefore improving both clinical pharmacodynamics bioavailability and specificity. In so doing, we also decrease off-target hits (in terms not just of receptors, but also of regionally delimited receptor sets) and both local tissue and systemic tolerance. The issue of cardiovascular and immune toxicity due to receptor effects distal to the therapeutically intended target tissues grows increasingly visible (Moslehi, 2016)
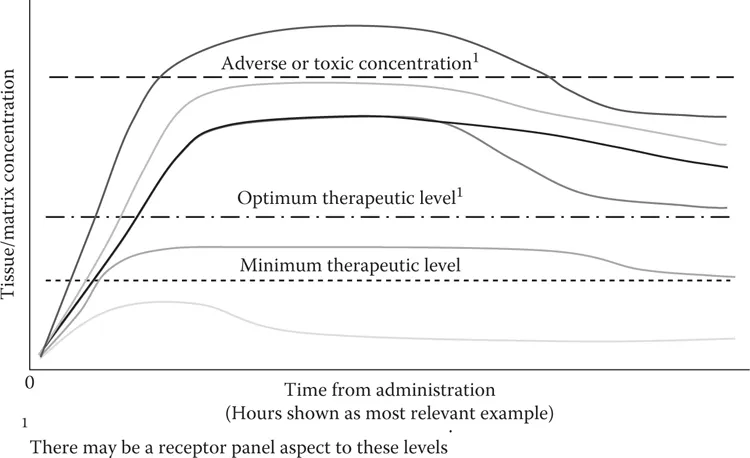
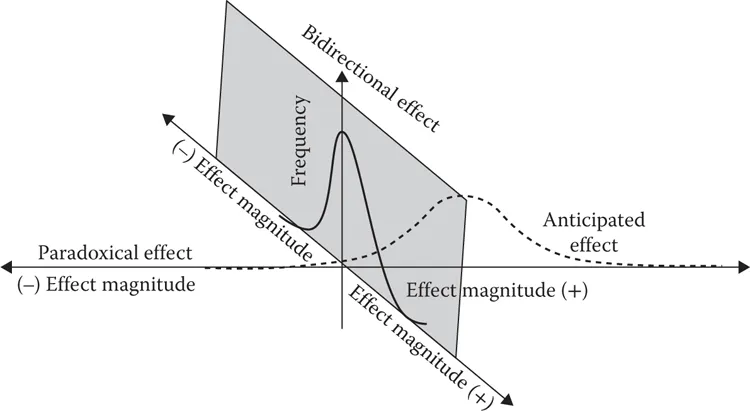
Our current model in pharmacodynamics is that we have a molecule which we want to adequately occupy a localized population of receptors so as to achieve our desired therapeutic effect (Keiser et al., 2009; Brunton et al., 2011). In this model, therapeutic efficacy is achieved by our drug molecules occupying target receptors for an optimal residence time period (Copeland, 2016). We have gotten very good at creating and identifying molecules to occupy specific protein receptors on a molecular level – but we must use animal models as surrogates to adequately understand how to do this on an intact higher-level organism and then be able to translate the findings to as close to an approval of human use methodology as possible before actually proceeding to humans. The common operating hypothesis is that if we get just enough test article to a target region, regardless of route, at sufficient plasma levels (minimum effective concentration, or MEC) while concurrently keeping Cmax levels of the test article in the plasma below a minimum adverse level (minimum toxic concentration, or MTC) in order to achieve ideal therapeutic efficacy and safety (and therefore, at unintended targets below MTC), we can achieve therapeutic perfection [Figure 1.1]). There is a balance that needs to be maintained with plasma levels: the presence of sufficient test article to achieve the maximum effect or efficacy coupled with consideration being given to not have plasma or desirable and undesirable tissue levels that are so high that the incidence and severity of adverse off-target side reactions are minimized. At the same time, there is a recognition that what are desirable therapeutic (and undesirable off-target) adverse – “toxic” – thresholds vary among individuals, particularly in the heterogenous human population (illustrated in Figure 1.2). One should note here an implication that the optimum concentration will usually not be at a level that requires occupancy of all target receptors.
FIGURE 1.1 Optimum therapeutic levels for tissue or minimum levels for effective and safe therapy.
As an essential part of progressing a potential drug to the point where its clinical attributes may be evaluated, the practicing toxicologist is faced with multiple challenges in developing formulations and optimizing routes and regimens for the evaluation of candidate drug formulations, which are not shared elsewhere in drug development. These challenges apply (with minor exceptions) across all routes of administration, for which intended clinical routes are preferred, if at all possible, to reduce the dimensions of extrapolation of results to the clinical use case:
FIGURE 1.2 Few drugs have a single effect profile - rather, there are usually both desired (therapeutic target tissue) and unanticipated (toxicity target tissue) effect profiles which overlap - or not.
• The components of formulations used to deliver a drug moiety must be tolerated – in multiple species (or duration of treatment) – while at the same time delivering plasma levels of candidate drug(s) that are of sufficient magnitude to please regulators. More than one formulation may be required over the course of development, each for a different species (or route).
• Nonclinical formulations are not required to be those used in clinical studies. Recent FDA expectations for dermal products have changed on this point, as there is also a desire for dermal systemic toxicity studies to imitate dermal transport metabolism and tolerance of a drug as it would be in use.
• Target doses that typically must be delivered are high – while volumes for delivery are limited to avoid inducing local tissue trauma in animals (“tolerance”).
• Tolerances of specific species to different vehicle components must be considered, and there is only limited literature available to help with this (Gad et al., 2016).
• Study durations may allow uses in early (short-term) studies that cannot be extended to longer studies.
• For most routes and studies, maximizing levels of solubility and systemic bioavailability and concurrently maintaining drug stability are primary objectives. In our experience, the implications of this may actually complicate or preclude successful development.
• With the general exception of the dermal route, rates of administration matter – and the regimens can be one of the tools of manipulation to achieve study goals.
• There are “points of art” which can be applied to most routes to help optimize the meeting of all these requirements mentioned above.
Receptor Theory of Drug Efficacy and Drug Toxicity
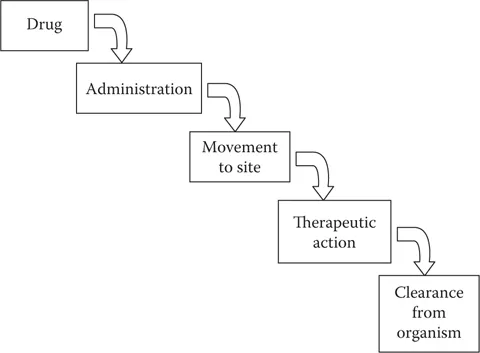
In 1906, Paul Ehrlich conceptualized the “magic bullet” approach to a perfect therapeutic, as introduced in Figure 1.3 (Drews, 2000). A perfect therapeutic would be specific to the target receptor and go in unmodified form to a target site in a patient, do what it needs to do, and subsequently leave or be eliminated from the body. Ehrlich was an immunologist seeking to treat infectious diseases and there was at that time no knowledge of proteins as receptors, but his vision has remained the ideal for pharmacotherapy. It turns out that things are just not that simple.
Our current working model in pharmacodynamics is still underpinned by Ehrlich’s model, being that we have one or more molecules which we want to adequately occupy a localized population of receptors so as to achieve our desired therapeutic effect (Keiser et al., 2009). The occupation may achieve its goal by either activating or blocking activation of receptors, or stabilizing them.
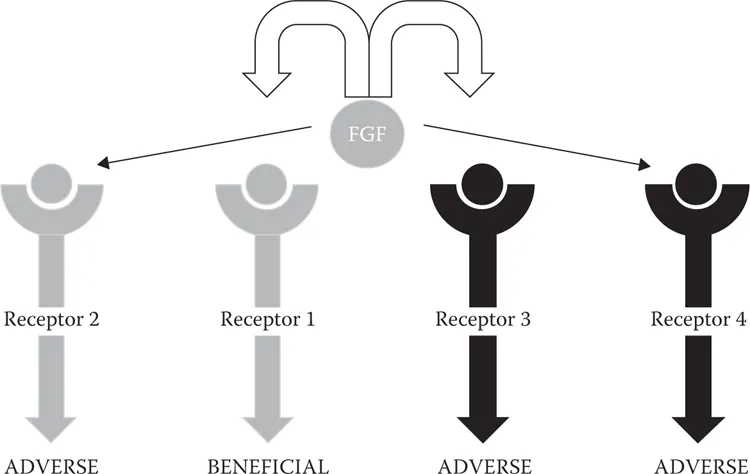
We have gotten very good at identifying molecules which occupy specific protein receptors on a molecular level – but we must use tissue and animal models to wholly understand how to do this adequately, with sufficient receptor and regional specificity to avoid adverse or even dangerous effects at an organism level and be able to translate the animal model to at least an approximation of human-use methodology before actually proceeding to humans. Figure 1.4 illustrates the concept of “off-target hits” for drugs – therapeutic molecules reaching unintended receptors at levels sufficient to activate them.
FIGURE 1.3 The magic bullet concept (Ehrlich hypothesis). Target sites are almost universally taken to be one or more forms of a protein or protein-complex receptor.
FIGURE 1.4 On- and Off-target effects.
As an essential part of nonclinical safety assessment, the practicing toxicologist is presented with multiple challenges in developing formulations for the in vivo evaluation of candidate drugs which are not shared elsewhere in drug development. These challenges apply, with minor exceptions, across all routes of administration. One of the ultimate goals is to determine, if at all possible, which use of the intended clinical routes is preferred to reduce the degree of uncertainty in extrapolation of results to the clinical use case.
Note that, however, where it is not possible to achieve a systemic exposure level by the intended route (not a rare case for topical routes), regulators may “recommend” use of a “systemic” route in an additional study to ensure that potential systemic adverse effects are identified and evaluated.
In the nine chapters that follow, we will seek to first assemble the basic concepts, principles, and hypotheses involved in quantitative receptor and chronological organism interaction dynamics central to the successful development of new therapeutics which depend on systemic administration to achieve desired therapeutic goals and in so doing avoid outcomes which limit, marginalize, or preclude the therapeutic use of so many molecules.
To do this we will first have to consider concepts central to current pharmacotherapy and toxicodynamics – and how current regulatory concepts and guidances hinder development but also could help improve the efficiency and success rate of development.
We will seek to understand the assumptions and concepts (and misconceptions) of (mostly nonclinical) pharmacokinetics. We both depend broadly on routes of administration to different species to give us accurate models by which to transfer therapies to humans (which largely disregard the differences of these species from humans, from one another, and between ages and genders in the model species).
Our technology and science have gifted us with many new tools and approaches to be able to more effectively and with specificity deliver therapeutic agents to desired targets, to guide them to targets, to activate and deactivate them when on target, and to quantitatively titrate their delivery to the target. Such delivery tools and approaches are overviewed in Chapter 5.
The concept of hormesis is a current version of the belief that dose responses (therapeutic and adverse) are not simply about “enough is better” but rather worse. There are, as illustrated in Figure 1.1, optimized levels.
Cha...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Dedication
Table of Contents
Preface
About the Author
1. Introduction
2. Pharmacotherapy, Toxicodynamics, and Regulatory Science: Divergent Objectives
3. Nonclinical Pharmacokinetics and Toxicokinetics: A Primer
4. Routes of Administration: With Considerations for Species Specificity
5. Delivery Systems
6. Dosing Regimens as a Means of Improving Drug Delivery and Tolerance
7. The Utility of Circadian Oscillations in Formulation and Drug Development Charles B. Spainhour
8. Fundamentals of Nonclinical Formulation: Chemistry and Biological Behavior
9. Vehicles and Excipients
10. Practical Ways of Improving Regional and Selective Drug Delivery
Appendix: Vehicles and Excipients
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Nonclinical Drug Administration by Shayne C. Gad,Charles B. Spainhour in PDF and/or ePUB format, as well as other popular books in Medizin & Pharmakologie. We have over 1.5 million books available in our catalogue for you to explore.