This revised textdescribes the theory substantiating adventure therapy, demonstrates best practices in the field, and presents research validating the immediate and long-term effects of adventure therapy.
A leading text in the field of adventure therapy, outdoor behavioral healthcare, and wilderness therapy, the book is written by three professionals who have been at the forefront of the field since its infancy. This new edition includes fully updated chapters to reflect the immense changes in the field since the first edition was written in 2010. It serves to provide information detailing what is occurring with clients as well as how it occurs.
This book provides an invaluable reference for the seasoned professional and is a required source of information and examination for the beginning professional. It is a great training resource for adventure therapy practices in the field of mental health.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Adventure therapy (AT), as it is defined in this book, is the prescriptive use of adventure experiences provided by mental health professionals, often conducted in natural settings that kinesthetically engage clients on cognitive, affective, and behavioral levels. Arriving at this definition was not easy, and it reflects the challenges faced by researchers, practitioners, and licensing and accrediting bodies in understanding a mental health approach that has largely been misunderstood and misinterpreted. On the one hand, AT is grounded in the Outward Bound Process Model, which was developed in the United Kingdom by the legendary Kurt Hahn. Outward Bound uses extended backcountry expeditions designed to challenge participants to overcome their perceived limitations and develop an enhanced sense of self and a sense of lifelong learning and mastery. On the other hand, AT could also use a challenge course as a tool to help families struggling with interpersonal dynamics develop new strategies to help them communicate with each other more effectively. It is for these and other reasons that multiple definitions of AT exist in the literature, leading to confusion on the part of researchers, educators, mental health practitioners, and others as to exactly what AT is and how it works to effectuate changes in individuals, groups, families, and organizations. The goal of this book is to address this ambiguity and to clearly and succinctly explore the history, evolution, theoretical foundations, current practices, and research on AT. In this revised edition, the goal has not changed, but it has evolved. There has been much debate about AT since the first edition was published, which we see as positive and necessary to move the field forward. A parallel goal of this revised edition is to address many of the discussions that emerged after the first edition of the book throughout our discussion about the history, theory, practice, and research in AT over the last decade. In this way, the authors hope to continue the discussion and dialogue that we hope illuminates the many ways AT can be delivered in North America and the world to clients in need.
The definition of AT remains a well-debated topic, if not a contentious one, due to multiple influences and widely varying applications. The evolution of AT in the United States and other parts of the world is well chronicled in Chapter 2, with key influences being early therapeutic camping approaches, the emergence of Outward Bound in the 1960s in the United States, and the increased need for alternative programs for youth in therapeutic and correctional settings. A systematic and integrated effort on the part of researchers and practitioners emerged from these influences to more clearly define AT and identify its key characteristics. Kelly and Baer (1968) demonstrated that a 21-day standard Outward Bound course for groups of adjudicated youth was more effective in reducing recidivism and less costly than traditional treatment for adolescents in a correctional program. Programs for adjudicated youth using the Outward Bound approach dramatically increased during this time. Providing additional insight into the work by Kelly and Baer (1968), Kimball (1983) discussed the power of wilderness for young offenders in the Santa Fe Mountain Center AT program. Gillis and Bonney (1986) provided one of the early rationales for using adventure activities in group counseling, and grounded their discussion of AT in the Outward Bound process (Bacon, 1983), and Project Adventure’s efforts to translate wilderness and adventure processes like Outward Bound into educational and counseling programs to be used in more urban settings (Rohnke, 1977). Gass (1993) followed these efforts by editing the first comprehensive text on AT and discussed seven key areas that provided the basis for AT: (1) action-centered therapy, (2) unfamiliar environment, (3) climate of change, (4) assessment capabilities, (5) small group development and a caring community, (6) focus of successful behaviors (strengths) rather than dysfunctional behaviors (deficits), and (7) altered role of the therapist.
In 1997, another important event occurred when the International Adventure Therapy Committee held its first meeting in Perth, Australia, with the proceedings edited by Itin (1997). In the introduction, Itin states “there is no universally accepted definition of adventure therapy, or of what constitutes it and how it is best conducted” (p. vi). Itin did provide parameters that framed the discussion as to how AT had been defined to that point, with narrow clinical definitions consistent with sister fields such as psychology, social work, and counseling on one end, and broader ones that believe AT could be any intervention that seeks to address maladaptive behaviors or support metalevel behaviors on the other end. Newes and Bandoroff (2004) later defined AT as a “therapeutic modality combining therapeutic benefits of adventure experiences and activities with those of more traditional modes of therapy” (p. 5) that integrates group-level processing and individual psychotherapy sessions as part of an overall therapeutic milieu. Newes and Bandoroff went on to discuss the implications of the debate, including asking questions as to what type of clinical and academic training best serves AT, as well as the need to explore the required qualifications and competencies of a practicing adventure therapist.
To this day, the debate and ongoing effort to define AT continues to cause a great deal of both semantic and professional confusion (Gillis, Gass, & Russell, 2008). Because of this, consumer groups, government agencies, academics, and professional councils have often created their own definitions. For example, the Bureau of Land Management (2008), which is charged with permitting programs to operate on public lands, defined wilderness/adventure therapy programs as “those programs intended to provide a less restrictive alternative to incarceration or hospitalization for youth who may require intervention to address emotional or behavioral challenges” (p. 1). The Council on Accreditation (2010), charged with accrediting and certifying AT programs operating in the United States, defined AT programs as “day or residential programs that provide an intensive, therapeutic experience based on outdoor, educational, clinical, and other activities that involve physical and psychological challenges” (p. 1). Although these definitions may suffice, the message sent to those interested in AT is clear: If we do not formally define AT ourselves, someone else may do so—and the definitions may be more harmful or distracting than they are constructive and focused. With a clarified definition comes acceptance by the medical establishment and third-party payers, making AT more affordable and accessible to families in need.
In July of 2016, the American Hospital Association recognized AT as a viable form of treatment, and the National Uniform Billing Committee in the United States established an insurance billing code for care (Gass, 2019). This update, and the corresponding change to the UB-04 billing manual, show that AT as an intervention has been recognized by both the general medical community and federal organizations as a valid treatment modality. Consequently, healthcare advocacy firms have helped implement the new revenue code advocating for families who are being denied coverage (“Outdoor/Wilderness Behavioral Healthcare, Revenue Code: 1006”). Denials Management, Inc., has reported that they have obtained over seven million dollars in reimbursements for families of AT between 2014 and 2018. They anticipate this amount to rise as the updated revenue code continues to pave the way for more widespread recognition of AT as a viable treatment alternative.
We therefore believe it is important to define AT and, in doing so, reference and pay respect to the key historical programmatic and individual influences and efforts that have shaped AT over the past decades. For this reason, the definition proposed at the beginning of this chapter aims to be a reference point for theory development, practice, and research. Key elements found in AT that differentiate it from, or link it to, other therapeutic approaches integrated into this definition include:
The intentional use of nature-based experiences.
Kinesthetic movement and physical exercise.
The involvement of meaningful and challenging adventure experiences for clients that facilitate experiential learning and natural consequences.
The use of eustress or the positive use of stress.
Healthy diet (especially on overnight or extended expeditions).
Screenless experiences.
The active and direct use of client participation and responsibility in their own therapeutic process.
Multidimensional and eclectic therapy.
The use of rituals and metaphor.
Practicing and developing mindfulness and reflection skills.
Solution orientation.
Harnessing the therapeutic power of group therapy and process.
This list is meant to serve as a starting point to discuss AT, not as a definitive inventory of AT foundational elements. Certainly, there are several other characteristics relevant to AT missing from this list; these are addressed elsewhere in this book in more detail. It is also important to note the use of the word prescriptive in this definition may raise some concerns among those historically involved with AT. We intentionally use this word to denote the ideally co-created way an adventure therapist (or treatment team promoting AT) would know their client (or client group) so well that an adventure experience would be tailored to the clients’ needs with full attention given to the clients’ affect, behavior, and cognitive abilities. We are not advocating a medical model in the pejorative sense; rather, we are advocating intention, co-creation, assessment, dosage, fidelity, and most of all the power to heal, restore, or prevent without doing harm.
We also are considering the changes in the role of the therapist in AT versus other “standard practices” psychotherapy. Adventure therapists actively design and frame adventure experiences around critical issues for clients, focusing on the development of specific treatment outcomes—and then get out of the chair! When utilizing adventure experiences with clients, adventure-based therapists are removed from serving as the central vehicle of functional change. The experience takes on the central medium for orchestrating change, freeing therapists to take on a more mobile role (e.g., for supporting, joining, confronting) in the co-construction of change processes with the client. Combined with the informal setting of adventure experiences, the dynamics of this approach remove many of the barriers limiting interaction. While still maintaining clear and appropriate boundaries, adventure therapists often become more approachable and achieve greater interaction with clients when compared to traditional therapists.
Adventure Therapy Practice
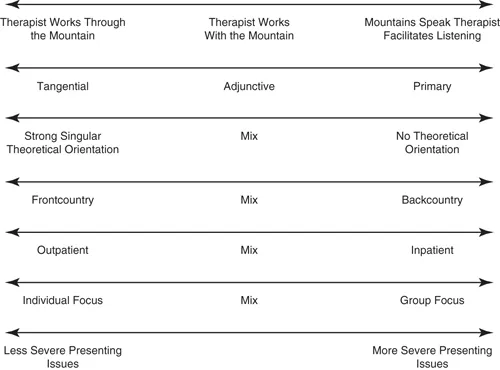
Rather than break AT into a typology based on various programmatic models, we believe that AT is better understood by exploring dimensions that help situate how AT is delivered by mental health professionals, programs, agencies, and managed care organizations. In this way, we hope to curb the confusion surrounding the definition debate, where AT has been referred to by a variety of terms, such as wilderness therapy, wilderness-adventure therapy, adventure-based counseling, adventure-based therapy, outdoor behavioral healthcare, wilderness challenge program, and wilderness experience program. As shown in Figure 1.1, these dimensions include:
Figure 1.1 Dimensions that help distinguish adventure therapy approaches.
1. The degree where the approach utilizes the “mountains speak for themselves” factor, in which nature plays a key therapeutic role in facilitating thought, reflection, and intended therapeutic change, or is facilitated more directly by the therapist.
2. The degree to which AT is viewed as primary, adjunctive, or tangential to the therapeutic process.
3. Practical linkages or theoretical connections to existing forms of therapy or treatment.
4. How and to what degree nature or wilderness environments are used.
5. The length or depth of the intervention in terms of time and resources allocated.
6. Individual- or group-based milieu used in treatment.
7. The severity of the client’s presenting issues.
The first dimension embraces the ongoing discussion of the powerful role that nature plays in AT, referencing the phrase coined by Rustie Baillie of the Colorado Outward Bound School when he famously said, “Let the mountains speak for themselves” (James, 1980, p. 1). The statement was made in reaction to a movement within Outward Bound circles to add an intellectual element to the courses through directed and guided facilitation of student experiences, rather than just letting the experience speak for itself and allowing participants to take from the course what they needed. In his famous essay on the subject, James captures the essence of the discussion in stating, “The experience happens naturally if instructors are skilled enough to take their students safely through the adventurous activities that make up Outward Bound, and when they do that, the mountains are extraordinary teachers indeed” (p. 1). Applied in an AT context, if therapists are working toward the “mountains speak” for themselves side of the spectrum, they allow the client to guide the process in reaction to what the environment and experience are providing for the client. If therapists tend toward the more active side, they will include interactive processes and work with or through the environment as a therapeutic tool and use the experience as a reflecting catalyst to help the clients integrate the experiences into their lives.
The second dimension refers to whether the use of adventure and activity is primary (i.e., first in importance and direct and immediate in its utilization), adjunctive (an additional component of treatment used in conjunction with more traditional models), or tangential (indirectly related to treatment and used more as a recreational outlet for clients). This dimension reflects the idea that adventure and activity, and their subsequent use varies widely across AT approaches and programs. In fact, this question was used on a survey of residential treatment programs in the United States (Russell & Gillis, 2010), where the majority indicated that adventure and activity were adjunctive (64.4%), with slightly over a third indicating primary (33.3%), and only 2% noting their use was tangential.
The third dimension refers to the degree to which the AT approach is grounded in traditional therape...
Table of contents
Cover
Half-Title
Title
Copyright
Dedication
Contents
Foreword
Preface
Acknowledgments
Authors
1 Introduction
2 A History of Adventure Therapy
3 A Psychotherapeutic Foundation for Adventure Therapy
4 Nature and Adventure Therapy
5 Foundations of Adventure Therapy
6 Assessment in Adventure Therapy
7 Practicing Adventure Therapy
8 Adventure Therapy Competencies
9 Supervision in Adventure Therapy
10 Research and Evaluation of Adventure Therapy
11 Risk Management of Adventure Therapy Programs
12 Adventure Therapy Ethics
13 The Future of Adventure Therapy
Appendix A: Risk Management of Adventure Therapy Programs
Appendix B: Adventure Therapy Competencies
Appendix C: Adventure Therapy Ethics
Appendix D: Research Rubric for Evidence-Based Research on Adventure Programs
Bibliography
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Adventure Therapy by Michael A. Gass,H.L. "Lee" Gillis,Keith C. Russell in PDF and/or ePUB format, as well as other popular books in Psychology & Mental Health in Psychology. We have over 1.5 million books available in our catalogue for you to explore.