Health Economics: An International Perspective is the only textbook to provide a truly international, comparative treatment of health economics. Offering an analysis of health systems across borders, the fourth edition of this key text has been updated and revised to take account of changes in a host of countries.
This edition features an expanded introduction, providing better grounding for many of the examples that come in subsequent chapters and making it easier for non-health care experts to see the links between the theory, the examples and the health care system components. It also boasts a restructured format, dividing the book into two broad sections: the first focuses on ideas and principles, along with evidence on their applications in the health sector, whereas the second focuses on introducing core tools and techniques used in applied health economics research.
Further updates to this edition include:
two new chapters on applied econometrics;
a new chapter on equity, focusing on equity in access to health care, paying particular attention to how access and need for health care are defined and measured in applied research;
a new chapter on emerging issues for health systems that are emanating from a series of global transitions both within (e.g. demographic change, epidemiological change, the global resolution on universal health coverage) and without the health sector (e.g. economic transitions).
Throughout the text, examples and illustrations are taken from a wide range of settings and world regions, providing a unique overview of the performance of different health systems.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Why do economists work in health? The health sector is not usually the first place people associate with economists. It is not supposed to be about money, profit, production and markets. Should it not be about medicine, nursing, caring and the difference between life and death? Surely, an economist has no wisdom to bring to bear here? Such views were virtually universal until quite recently but they demonstrate a limited understanding of the role and content of economics. In principle economists are concerned with better choices and in particular making the best use of existing resources and growth in the availability of resources. As economists started to work on problems in the health sector, the new discipline of health economics emerged. Many of the concerns in health economics are also those of other health scientists – how can we improve survival, quality of life and fairness in access to services? What economics brings is a different framework for analysing such questions. We think this framework offers important and useful insights.
Economists in all sectors are concerned with the allocation of resources between competing demands. Demands are assumed to be infinite – there is no end to consumption aspirations. Resources (like labour, raw materials, production equipment and land), in contrast, are always finite. Thus scarcity of resources (not in the sense of ‘rarity’ but in the sense of resource availability relative to demand) becomes the fundamental problem to which economists address themselves. Some readers will have difficulty with this description of the world. It is not necessarily ‘true’ but is, in a broad sense, a model on which economics is based. See Box 1.1 for further discussion of the nature and purpose of models, and of this one in particular.
Box 1.1Realism and the need for simplification – the use of models in economics
In the teaching of health economics, we have found that students often raise objections to the assumptions of economic models and the characterisation of all-pervasive scarcity on which economics is based. Others object to the concept of the ‘rational economic man’ that underlies demand theory (see Chapter 2), and the assumptions of the theory of perfect competition (see Chapter 6).
At least part of the concern comes from a misunderstanding of the role and usefulness of theories and models. Models are not intended to describe reality. They deliberately abstract from it, in order to simplify the relationships between key variables so that we can see them clearly and analyse them. Models should never be ‘realistic’, they should always be simplifications. Models deliberately ignore variables we are less interested in, or consider to play only a small role, either by holding them constant or by setting them to zero. Economists use the expression ‘ceteris paribus’ (all the rest the same) to indicate that all variables which haven’t been included in the model should be assumed to be constant. By simplifying, we aim to focus on the relationships we are interested in, examine the interactions between these variables, and avoid the ‘noise’ of the hundreds of other variables which will otherwise confuse those key relationships. An extreme position is that of Milton Friedman (1953), who has argued that a model is good if it predicts accurately. Its assumptions may bear no relationship with reality. Friedman uses the example of leaves deliberately seeking to arrange themselves so as to maximise the sunlight each receives. The assumption of ‘deliberating’ leaves may be unrealistic, but a model based on that assumption predicts accurately the pattern of leaf growth and development on a tree. Others (e.g. Hodgson 1988) consider that a model which predicts on the basis of very unrealistic assumptions fails to explain the relationships in question. We do not understand much about the process of leaf growth and distribution starting from this assumption. Explanation is often as useful a function of models as prediction.
Take the particular assumption that demands are ‘infinite’. Are they really? Levels of consumption enjoyed in the rich economies of the world have grown beyond the imaginations of previous generations. The consumption levels of the richest in the world demonstrate that when resource constraints are low, people consume goods that would in other circumstances be considered of very low priority. If demand exists for psychiatric services for pet dogs, cars capable of speeds exceeding the maximum permitted on public roads, and dancing snowmen singing ‘Jingle Bells’, where can limits be found? Observing some spectacles of consumption, one might conclude that increased wealth and command of resources increase greed and aspirations to consume even more.
In the health sector, one might reach similar conclusions based on the rapid development of technology, which makes available almost unlimited opportunities to extend and improve the quality of life. There seems no limit to the resources that might be consumed with the objective of improving the health of a population.
However, it is also clear that not all members of the world’s population aspire to such levels of consumption. Many widely held systems of philosophic and religious belief from Calvinism to Islam eschew consumerism. And even if the levels of demand which might potentially be expressed are very large indeed, could they really be infinite? Is there not a maximum rate at which any individual could possibly consume resources?
The discipline of economics needs an assumption which is realistic enough to generate useful analysis and conclusions. What is unarguable, is that the extent of demands on resources far outstrips the capacity of available resources to deliver, and does so to such a great extent that there is no prospect of ever meeting all demands with the available resources. This is sufficient to make the economist’s characterisation of all-pervasive ‘scarcity’ a reasonable basis on which to proceed.
Of course, the current distribution of resources leaves some high-priority demands unmet at the expense of some of the low-priority demands listed above. For the cost of the dancing snowman, several people might have their sight restored through cataract surgery. In this insight lie the concerns of economists. Why do the current resource allocation mechanisms choose snowmen over cataract surgery? If we take the normative perspective that surgery is ‘better’ than snowmen as a starting point, what kinds of intervention might help us move towards a situation in which more demands for surgery and fewer demands for snowmen are met? These questions are the business of economics.
In the health sector, such scarcity can be recognised in a host of questions that concern all who work there or use its services. Why has the volume of resources absorbed by the sector increased so fast over the last four decades worldwide? Why does it seem that no matter how many nurses and doctors are employed, new technologies adopted, new drug therapies introduced, even the rich countries of the world do not seem to be able to provide the highest quality of care for all citizens? Are we investing in the wrong kinds of health services? Are we organising services so as to best improve the health of the population? Are we investing in technologies that have a low health output compared with alternative investments? In poor countries, questions of resource scarcity are starker still. Can we afford, at all, universal access to high-cost services such as cancer care?
All societies must make choices as to how to allocate whatever resources are available to the production of health services, and how to distribute those health services. These choices are the subject of the discipline of health economics. Health economics (and economics in general) is often seen as having two branches: the positive branch, which is concerned with describing and explaining how such choices are actually made; and the normative branch, which is concerned with judging which choices should be made. For example, a health economist might be concerned with the health insurance coverage of a population. She might take a positive perspective. Why are there so many uninsured? What are the characteristics of those that are uninsured (are they unable to afford the cost of insurance premiums, or do they judge themselves unlikely to need health services)? From a normative perspective it is necessary to establish criteria according to which the situation can be judged. If equity of access to health services is one criterion, and inability to pay is a dominant explanation of non-coverage, the situation might be judged ‘bad’, and alternative interventions to reduce the problem evaluated.
1.1.2 Planned versus market – alternatives for organising resources
There are two ways in which society can make choices about the collection of resources and allocation of resources to production in the health sector, and the distribution of the services that are produced among those that want them. A society can leave these decisions to the market – letting demand, supply and prices determine resource allocation – or it can plan, usually by giving its government the task of collecting resources from the population, allocating those to defined production activities and distributing the produced services among the population.
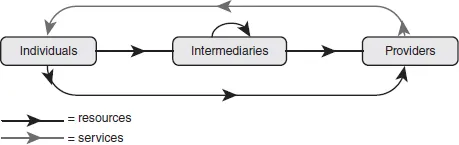
Figure 1.1 gives a stylised overview of the structure of a health care system. The diagram shows the flow of resources (black arrows) and services (grey arrows) through any health sector. Ultimately, resources from individuals in society are used to pay, either directly or via intermediaries, providers such as primary care providers or hospitals to deliver health care services to individuals in society.
Figure 1.1Flow of health care resources and services
Source: Brick et al. (2010).
Describing the above choices in terms of Figure 1.1, where society leaves the decisions to the market, resources flow directly from individuals to providers (i.e. bottom black arrow) who in turn produce health care for those who are willing to pay at that market price. In a planned health care system, resources are collected from individuals by an agreed intermediary (e.g. government tax collector, social health insurance fund), which in turn pays providers (e.g. via annual budgets, capitations, or fee-for-service) to deliver health care services in accordance with specified health care delivery principles (e.g. services allocated on the basis of need).
The debate as to which approach is best has divided the world’s population through the whole of the twentieth century, underlying the formation of political parties, coups d’état, and hot and cold war, and will not be settled in this volume! Societies worldwide have taken different stances on the question, and have evolved a wide array of mixes of plan and market in the attempt to reach a satisfactory choice as to how to produce and distribute health services. Thus, even in the most highly planned health systems, market forces can be found to operate in some parts of the system, for example for specific services (e.g. a market for drugs for which prescriptions are not required operates in almost all countries), or for specific groups in the system.
Health economists have evolved different approaches to analysing and evaluating resource allocation in the health sector which reflect the plan–market dichotomy. In societies in which health services have been largely planned (e.g. Europe), the main activity of health economists has been the development and application of a set of tools which collectively make up the field of economic evaluation. Economic evaluation aims to consider whether appropriate services have been adopted in the health sector, or whether there is a mix of technologies and interventions which would better meet health sector objectives, such as the improvement of the population’s health, or the equity of access to care. You might notice that in terms of the positive–normative dimension, this is an essentially normative activity. It requires the definition of objectives and asks: ‘What should we do?’
Where there has been a greater role for the market in health sector resource allocation (e.g. in the United States), more effort has been made by economists to understand that market in order to predict its pattern of development, and to analyse the implications of interventions such as regulation, subsidy of insurance coverage or the introduction of planned activities. Even in the most market-reliant health sectors, such interventions are always present. Understanding markets involves the understanding of demand (how consumers of health services express their preferences through their ability and willingness to pay), supply (conditions in input markets, cost and how provision is organised, e.g. by one big firm or by many) and their interactions. This is essentially a positive activity – explaining what is happening and predicting the effects of introducing a change – but it can be normative. If it is decided that a particular effect is desirable, such analysis can be used to evaluate whether a change should be introduced.
As health sectors have evolved, especially over the last two decades, richer mixes of planning and markets have been developed in a large number of countries. In health sectors which have traditionally been planned, elements of market mechanisms have been introduced, for example through ‘internal markets’ (i.e. focusing on the interaction between intermediaries and some providers, see Figure 1.1). In health sectors which have traditionally relied to a greater extent on market mechanisms, more planning has been introduced – for example through more intrusive public regulation, or through the use of capitation payment mechanisms (consumers pay the provider a fee per year rather than per service) which shift risk on to providers and thereby pass on the planning role usually carried out by a public sector body. This has led to a certain cross-over of interests in the health economics fields. US health economists are now much more interested in the techniques of economic evaluation which can assist Health Maintenance Organisations (providers paid by capitation) in developing their strategies, and economists interested in the welfare state health provision of northern European countries are increasingly interested in the operation of markets and the implications of different kinds of regulation and other public intervention for market behaviour. On both sides of the Atlantic there is now interest in capturing the insights of economic evaluation to enable better planning by actors in the market place, and to better understand how public intervention can improve outcomes associated with health markets.
These two traditions of health economics can be detected by comparing the outputs of health economists in northern Europe, Australia and New Zealand (largely planned health sectors), and the United States (where market forces have been allowed greater rein). Canadian health economics has perhaps been least categorisable, located in a health sector which is characterised by planned approaches to resource allocation, but strongly influenced by the academic environment of the United States. Some prominent contributions to health economics from Canada have provided a critique of US analysis.
Although most work in health economics has been produced in these regions, trends in health sector development affect those conducting economic analysis in the health sectors of almost all countries. It is no longer safe to assume that when one is working in a planned environment, an understanding of market forces is unnecessary, and that topics in economic evaluation provide the only useful tools required. Similarly, it is unlikely that the United States will ever return to the market conditions of the 1970s. Technology assessment, facility planning and the mandate of insurance packages are likely to feature for the foreseeable future, and economic evaluation will continue to play a major role in the operation of these.
It is therefore increasingly the case that, wherever their work takes them in the world, a health economist needs grounding in both branches of the discipline. This book is founded on that belief. It aims to explain basic health economics across the spectrum of the discipline and to demonstrate applications on a worldwide basis. The work of the authors of this book covers a wide geographic span, taking in Western Europe, the United States, Canada and Australia, many of the countries of the former Soviet Union and Eastern Europe, Uganda, Zambia and Zimbabwe, Bangladesh, Cambodia, India, Colombia and Peru – in fact countries from all continents except Antarctica. Obviously, the problems faced by these different countries in trying to ensure that public health problems are thoroughly addressed and that all citizens receive high-quality health services are quite different – in type and degree. Nevertheless, the tools of economic analysis presented in this book have provided us with a good basis for seeking to understand and evaluate the problems encountered and the measures taken to respond to them irrespective of the context. We believe that contrasting experience of applying these tools in different countries is helpful in understanding issues and undertaking analysis in any particular country. The aim of this book is to provide an introduction to these tools and to show ways that the same approach can inform health policy in widely differing contexts.
1.2 Who and what is in a health system?
Much of this book is concerned with introducing the reader to the workings (and failings) of markets in the context of health care. Markets are made up of different actors and it is useful to set out here the key players in a health care system because these crop up throughout the text, wherein core ideas and theories are illustrated using examples from existing health care systems.
Figure 1.1 id...
Table of contents
Cover
Half Title
Title
Copyright
Contents
List of figures
List of tables
List of boxes
Preface to the fourth edition
1 Introduction: health economics in international perspective
Part I Introductory health economics
Part II Further economics of markets and market intervention
Part III The economics of health systems
Part IV Tools and techniques for measurement and analysis
Part IVa Economic evaluation
Part IVb Applied econometrics and other tools
References
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Health Economics by Barbara McPake,Charles Normand,Samantha Smith,Anne Nolan in PDF and/or ePUB format, as well as other popular books in Medicine & Finance. We have over 1.5 million books available in our catalogue for you to explore.