- 266 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
ENT emergencies are a regular occurrence. This new book covers the full range of hospital emergencies seen by ENT trainees and practitioners, and also by oral and maxillofacial surgeons and plastic surgeons. Succinct text and clear illustrations complement the sections on Rhinology,Head and Neck,Otology and Paediatrics.Practical and up to date, this book facilitates excellence in clinical practice.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1Emergencies in Rhinology
1Epistaxis
Iain Hathorn
2Acute severe rhinological infection
Wai Keat Wong and Salil Nair
3Acute CSF rhinorrhoea
Quentin Gardiner
4Management of acute nasal trauma
Richard Green and Peter Ross
5Management of orbital injury and expanding orbital haematoma
Bridget Hemmant and Carl Philpott
6Emergency management of the complications of infective sinusitis
Andrew C Swift
7Nasal foreign bodies and rhinoliths
Catriona M Douglas and Brian Bingham
1Epistaxis
Iain Hathorn
Introduction
Management
Primary epistaxis
Secondary epistaxis
Key learning points
Further reading
Introduction
Epistaxis is defined as bleeding from the nose and is one of the commonest emergencies dealt with by the otolaryngologist. The overall incidence of epistaxis in the general population is difficult to determine because most cases are unreported, minor, self-limiting episodes or those controlled with simple first-aid measures. Fewer than 10% of patients seek medical attention for epistaxis and fewer than 10% of those requiring hospitalisation require surgical intervention for control of bleeding.
Due to the fact that many cases involve the elderly population, epistaxis is a significant cause of morbidity and even mortality in general otolaryngology practice. In England there were 22,671 admissions in 2014/2015, with a mean stay of two days.
The nose has an excellent blood supply from both the internal and external carotid arteries, which anastomose extensively within the lateral wall of the nose and septum. The external carotid artery supplies the nose via the facial and maxillary branches. The maxillary artery supply is via the sphenopalatine and greater palatine branches and the facial artery supply is mainly via the superior labial artery. The sphenopalatine artery is the most important blood supply to the nose and it enters the nose via the sphenopalatine foramen before dividing into the posterior septal artery, which runs medially across the face of the sphenoid to the posterior septum and subsequently Little’s area, and the posterior lateral division, which supplies the inferior and middle turbinate. The internal carotid artery contributes the anterior and posterior ethmoid arteries via the ophthalmic artery, and supplies the superior part of the nasal septum and lateral wall.
Epistaxis can be classified anatomically into anterior (Kiesselbach’s plexus) (Figure 1.1) and posterior (Woodruff’s plexus) (Figure 1.2). Kiesselbach’s plexus (or Little’s area) is an arterial plexus on the anterior nasal septum and is a frequent site of bleeding. Woodruff’s plexus is an area of prominent blood vessels lying just inferior to the posterior end of the inferior turbinate. This is a common site of epistaxis in adults. Perhaps a more useful classification, which has the advantage of guiding management, is based on aetiology and whether the epistaxis is primary (80%) or secondary (Table 1.1). Twenty percent of cases will be classified as secondary epistaxis with a local or systemic cause identified. There are also aetiological associations with epistaxis. These include septal deviations and spurs that disrupt normal airflow, causing dessication, increased mucosal fragility and epistaxis. Septal perforations often result in the formation of granulation tissue and crusting, due to the lack of epithelium covering the margins, which can result in epistaxis. Alcohol can affect bleeding time, even when platelet counts and coagulation factors are normal. Epistaxis patients are more likely to consume alcohol than matched control patients and are also more likely to have hypertension. Long-standing hypertension may result in vascular fragility from long-standing disease; however, it is rarely a direct cause of epistaxis.
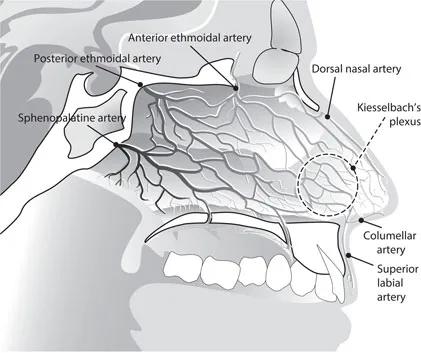
Figure 1.1The vascular supply of the nasal septum and locus Kiesselbach’s plexus.
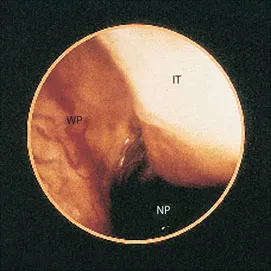
Figure 1.2Endoscopic photograph of Woodruff’s plexus. WP-Woodruff’s Plexus, NP- Nasopharynx, IT-Inferior Turbinate.
Table 1.1Aetiology of epistaxis
Idiopathic | 80% of cases |
Trauma | Digital, external, nasal trauma, iatrogenic |
Coagulopathy | Idiopathic thrombocytopaenia (ITP) Disseminated intravascular coagulopathy (DIC) |
Drugs | Warfarin, aspirin, clopidogrel, apixaban, dabigatran, rivaroxiban |
Chronic granulomatous disease | Granulomatosis with polyangiitis, sarcoidosis |
Neoplastic | Angiofibroma, inverted papilloma, squamous cell cancer |
Hereditary | Hereditary haemorrhagic telangiectasia (HHT), haemophilia, von Willebrand’s factor deficiency |
Management
Primary epistaxis
Assessment and resuscitation
The patient presenting with epistaxis should be assessed as per Acute Life Support guidelines (Airway, Breathing, Circulation). They should be sitting up and leaning forward, with pressure applied to the anterior part of the nose by pinching continuously for 10 minu...
Table of contents
- Cover
- Half Title Page
- Title Page
- Copyright Page
- Contents
- Contributors
- Section 1 Emergencies in Rhinology
- Section 2 Emergencies in Head and Neck
- Section 3 Emergencies in Otology
- Section 4 Emergencies in Paediatric ORL
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access ENT, Head & Neck Emergencies by S Musheer Hussain in PDF and/or ePUB format, as well as other popular books in Medicine & Ear, Nose & Throat Medicine. We have over 1.5 million books available in our catalogue for you to explore.