This accessible book offers effective protocol for engaging in better sexual decision-making in clinical practice. It demonstrates that damaging sexual behaviors are often the result of a process in which a clinician progresses towards the crossing of a client-clinician boundary.
Sexual Attraction in Therapy explores state-of-the art research from a multitude of related fields and includes sage advice on how to recognize personal risk factors, manage arousal, identify counterproductive sexual behaviors, and use self-talk to exit sexual situations. Sexual boundary violations usually follow a much longer insidious process and the book carefully discusses and highlights the warning signs for clinicians, which can develop into sexual predicaments affecting their lives and those of their clients, their workplaces and colleagues, and the reputation of the mental health field. Chapters provide essential guidance so that therapists can monitor progress along the 'sexual decision cycle' and, importantly, create organizations far more resistant to poor sexual decision-making.
This text is an excellent teaching guide for clinicians and treatment professionals who seek therapeutic growth for both clients and themselves. Clinicians will be able to improve their decision-making and prevent themselves from engaging in damaging sexual behaviors, and organizations can redesign their approach to include preventative practices.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
In 1989, Robert Simon’s seminal article “Sexual Exploitation of Patients: How it Begins Before It Happens” was published in Psychiatric Annals. The author concluded sexual boundary violations were not sudden events but rather the results of a gradual and imperceptible process, and he offered the following vignette to illustrate his contention:
A 48-year-old male therapist began individual insight psychotherapy of a 29-year-old woman who was attractive, divorced, and depressed. The psychotherapist recently had concluded a bitter divorce after 20 years of marriage. For about six months, the therapy progressed with treatment boundaries intact. Then, gradual incursions began. The therapist and patient began to address each other by their first names. The tenor of the therapeutic sessions increasingly became more social with mutual sharing of experiences. For example, on one occasion, the psychiatrist talked about his divorce and his loneliness. The patient responded by describing the various social functions available to divorcees. At the beginning of treatment, sessions were originally terminated in a verbally appropriate manner. However, over time, a handshake at the end of the session progressed to a hug. Initially, the hugs were perfunctory, but therapist and patient began to linger in their termination embraces. In due course, the therapy sessions were rescheduled for the end of the day. Before long, therapist and patient occasionally dined together. Movie dates followed where hand-holding and kissing took place. Eventually a sexual relationship “happened.”
(pp. 105–106)
Now, more than three decades later, the same step-wise progression from therapy to sex, built upon what Simon calls a “culmination of many earlier incursions into the treatment process” (p. 106), occurs in current cases of sexual boundary violations. The above example could be easily modified to fit the modern age with inclusion of a sentence about texting and social media as conduits of communication between sessions by both professional and patient. Other than rape in a therapy context – a rare occurrence – sexual boundary violations are the end result of an extended process, whether the involved professional is a psychologist, counselor, therapist, or social worker.
Simon and those that followed determined that there are key features of therapy that facilitate the progression from well-intentioned professional therapeutic work to a sexual boundary violation. These characteristics are so common that they led Honig and Barron (Honig and Barron, 2013) to conclude that for those in the mental health treatment field “boundary violations is a shared occupational hazard” (p. 901).
The Inherent Risks of Therapy
Sexual attraction and arousal are parts of the human condition and will inevitably find their way into the consulting room. This is to be expected and not a need for embarrassment. Neither should they be ignored; as such, learning how to manage arousal and attraction is a core theme of this text.
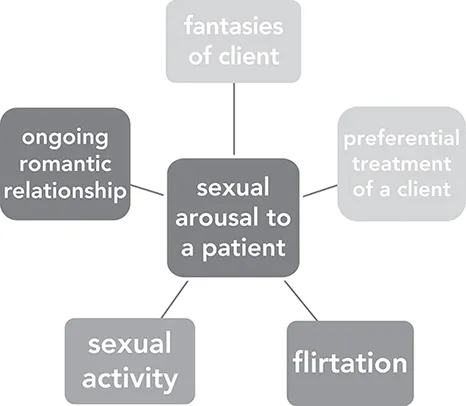
Attraction and arousal in clinical settings tends to manifest in five ways, as illustrated in Figure 1.1. While practitioners will agree that flirtation, sexual activity, and romantic relationships with clients are clearly wrong, this text will show that even fantasies and preferential treatment can have consequences.
Figure 1.1 The Manifestations of Sexual Arousal in Clinical Settings
What about the mental health treatment field leads to the shared occupational hazard of boundary violations? First, and above all else, a therapeutic relationship is a unique form of personal interaction that fosters attraction and arousal. According to Schwartz and Olds (2002), there are six reasons for this common outcome.
Patients often begin treatment when other relationships in their lives are dissatisfying or dysfunctional. As such, mental health professionals enter a client’s life when the latter are most susceptible to attraction to a person who genuinely cares about them.
Mental health practitioners experience undulations in their own relationships, including romantic relationships, and need for intimacy themselves; when a therapist is lonely or romantically discontented there will always be appealing and willing patients who could satisfy these desires.
Unconditional positive regard, while a recognized crucial ingredient for treatment, paradoxically increases risk for attraction; according to the authors, “The degree of unwavering attentiveness to the patient’s thoughts and feelings, to the nuances of the patient’s words and gestures is not likely to be matched by the best of lovers or friends over the long haul. The fact that the therapist only sustains that selfless attention over a 50-minute session is too often neglected by both participants” (Schwartz and Olds 2002, pp. 485–486).
Therapy aims for ever-increasing levels of intimacy. Even cognitive therapy, an approach not traditionally thought of as entailing profound intimacy, enjoins clients to move beyond an exploration of overt behaviors to underlying automatic thoughts and finally onto their unspoken and implicit core beliefs. Therapy is a progressively intimate experience.
Limited self-disclosure by practitioners leads some patients to an extended idealization of them; they never have the opportunity to see the deficits, flaws, and frustrating aspects of a mental health worker’s personality that is so readily apparent to their romantic partners, friends, and children.
Treatment is conducted without witnesses. Not only does this lead to a lack of surveillance as to what is actually happening behind closed doors in sessions, it also leads to emotional deprivation in existing relationships. Professionals, due to confidentiality laws, are unable to share major portions of their lives with loved ones, and clients, in turn, withhold their most intimate thoughts and feelings from others in their lives, which are only revealed in therapy sessions. This secrecy prevents concerned others from recognizing that a therapeutic relationship is devolving into boundary violations. According to Schwartz and Olds (2002),
“Not only is the connection between therapist and patient hidden away from the potentially beneficial gaze of others who care about the patient. The patient’s relationships with these others are devitalized by siphoning off from them the patient’s most heart-felt concerns. When what is most vivid in our lives is not shared with those we love, our connection with those we love becomes impoverished. That impoverishment is a serious concern for patients and therapists alike. When we live a significant part of our lives without witnesses, we deprive ourselves of more than just a policing presence … Psychotherapy is a relationship uniquely designed to maximize the experience of interpersonal “flow” within it, while simultaneously insulating both participants from the scrutiny and jealousy of lovers and friends that might act as natural breaks on progressive intimacy.
(p. 490)
Psychological Risks
All clinicians at some point in their career will experience sexual fantasies or sexual attraction towards a client or will be the object of a client’s erotic attention. As noted above, the dynamics of therapy ensure this occurs. Still, clinicians tend to underestimate the power of attraction and often deny the possibility that this will even happen; they convince themselves that they are somehow immune to arousal and attraction in clinical settings. Of course they have no reason to doubt this since the majority of practicing professionals report their formal university training did not prepare them for sexual arousal in the clinical realm. Pope, Keith-Spiegel, and Tabachnick (1986), as one example, surveyed psychotherapists about experiences of sexual attraction to clients. Responses indicated that half of the respondents did not receive any guidance or training concerning this issue, and only 9% reported that their training or supervision was adequate. Finally, those who have been practicing in the field for an extended period of time believe they are resistant or even immune to sexual attraction and the risk of dual relationships.
Three psychological factors reinforce the common underestimation of risk for engagement in a sexual boundary violation:
the fundamental attribution error;
splitting; and
believing current preventative measures are sufficient and as such nothing else can be done to decrease risk.
The Fundamental Attribution Error
The fundamental attribution error, a concept that came into common parlance by Ross (1977), states that we have a cognitive disposition to overemphasize personal characteristics and ignore situational factors when judging others’ behavior. Thus a person’s “bad” behavior reflects their true underlying personality; situational factors are disregarded. Professionals and the organizations in which they practice configure transgressing clinicians as “bad apples,” mistakenly hired into the field and who need to be removed as quickly as possible. Even more, these boundary violating clinicians are perceived as irredeemable and beyond the efforts of any form of rehabilitation. Circumstances leading to a boundary violation are elided regardless of the fact that situational antecedents always occur. Smart, compassionate, and empathic people do not destroy their lives and that of involved patients without specific situational factors insidiously motivating behavior. Through use of the fundamental attribution error however, clinicians can rest easy believing they would never engage in the same behavior and that there must be something seriously wrong with those individuals allowing it to occur. These former clinicians underestimate the influence and outright power of situational factors and discount the possibility that they too could be swept up into a boundary violation.
Splitting
The second reason clinicians ignore risk builds upon the fundamental attribution error, and this is the well-known defense mechanism of splitting, which allows us to divide people or beliefs into good or bad and positive or negative. Upon learning that a current or past colleague, a trusted professor, or a well-respected leader in the field has engaged in a sexual boundary violation, the mind, unable to tolerate uncertainty and hold opposing ideas (i.e., a person I trust and admire engaged in unethical and injurious behavior), overcomes the complexity by simply allowing us to focus on only the bad aspects of the transgressor. We immediately and harshly judge clinicians engaging in sexual boundary violations as evil, nefarious, incompetent, damaged, and/or sick. While it would be comforting to conclude that offending professionals have severe characterological problems, the research is very clear and finds a far more worrisome conclusion: risk is based on an ever-changing conflux of clinician characteristics, client characteristics, the nature of the therapeutic relationship in general, an agency’s milieu, supervisory relations, even unconscious factors. Still, professionals of all disciplines minimize or outright deny this risk. It is so much easier for the human brain to simply ignore all of these factors, deride the transgressing clinician, and move on with hubris that “I” would never engage in similar behavior. We see here a split into the ubiquitous “us and them” with “us” as the good clinicians and “them” as transgressors; splitting allows clinicians to ignore their idiosyncratic risk since they do not perceive themselves as being in the same category as transgressing professionals.
Believing Current Preventative Measures Are Sufficient
Clinicians believe current preventative measures are successful or at least cannot be improved upon. Mental health treatment facilities, licensing boards, and professional associations have done what they can to prevent sexual boundary violations. During their university training, prospective mental health professionals learn that sexual boundary violations are never justifiable. They later sign ethical statements reiterating this directive as part of their licensure process as well as when voluntarily joining professional associations. Annual or bi-annual ethics trainings, a mandatory requirement for professionals to maintain licensure, continue to stress the edict prohibiting dual relationships. Professionals understand their behavioral restrictions and partake of existing preventative measures; what more, they think, can I do?
The Six Pillars of Prevention
How do we navigate the inherent risks of therapy, our complacency, and a tendency towards self-deception? We will make little progress until we outright acknowledge four conclusions about sexual violations occurring in the mental health treatment field.
First, it is difficult to eradicate behavior that is purposefully secreted. The antecedents leading to a sexual boundary violation as well as the violation itself take place within the parameters of private therapy sessions, in which knowledge and oversight of what is actually occurring behind closed doors is minimal to non-existent for outsiders. According to Gabbard (1996),
“Among the many ironies of the practice of psychotherapy is that the privacy of the confidential therapist-patient relationship is both the cornerstone of practice and a major risk factor in the development of boundary violations. What transpires in psychotherapy is not observed by anyone other than the two participants.”
(p. 316)
Furthermore, a violating clinician frequently manipulates the client into moving their clandestine relationship into other domains to avoid detection; this stealthy maneuvering is very similar to the precautionary measures used to hide an extramarital affair.
Second, sexual boundary violations continue to occur because of shared silence by all involved parties and witnesses. Offending clinicians and their client victims are unlikely to self-disclose a sexual boundary violation. The transgressing clinician is of course fearful of consequences, and clients often report they have fallen in love and do not want to hurt their new lover who was in the not too distant past their mental health professional. Other clients are so confused by the experience that they simply do not know how to respond. Those experiencing power differentials between themselves and a c...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Dedication
Table of Contents
Introduction: An Overview of the Problem
1. A Roadmap for Navigating the Risks of Therapy
2. The Boundary Violation Cycle
3. Risk and Vulnerability Factors
4. Managing Fantasies
5. Choosing: Talking Ourselves into (and out of) Sexual Predicaments
6. Using Clients to Meet Unfulfilled Needs
7. Non-Sexual Boundary Crossings
8. Violations and Post-Violation Considerations
9. Education, Training, and Supervision
10. Organizational Change
11. Removal or Rehabilitation
Conclusion: We’re All in This Together
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Sexual Attraction in Therapy by Michael Shelton in PDF and/or ePUB format, as well as other popular books in Social Sciences & Education in Psychology. We have over 1.5 million books available in our catalogue for you to explore.