The Psychology of Eating is the essential multi-disciplinary introduction to the psychology of eating, looking at the biological, genetic, developmental, and social determinants of how humans find and assimilate food.
Thoroughly revised and updated, the new edition brings multi-faceted expertise to the topic of normal and dysfunctional food intake, juxtaposing "normal" eating, eating in environments of food scarcity, and the phenomenon of "abnormal" eating prevalent in many modern-day developed societies. Eating disorders are not a focus, but also emerge from, this approach. Key features include:
A new expanded section considering the roles of business and government in creating and potentially solving the issue of "abnormal" eating
Learning objectives, talking points, and end-of-chapter glossaries
Chapter-by-chapter self-assessment questions.
With questions of food production, food choice, and environmental sustainability becoming more critical in an increasingly populated world, this is crucial reading for undergraduate courses in Psychology and other disciplines with a holistic and critical thinking approach to the psychology of food intake.
Frequently asked questions
How do I cancel my subscription?
Simply head over to the account section in settings and click on “Cancel Subscription” - it’s as simple as that. After you cancel, your membership will stay active for the remainder of the time you’ve paid for. Learn more here.
Can/how do I download books?
At the moment all of our mobile-responsive ePub books are available to download via the app. Most of our PDFs are also available to download and we're working on making the final remaining ones downloadable now. Learn more here.
What is the difference between the pricing plans?
Both plans give you full access to the library and all of Perlego’s features. The only differences are the price and subscription period: With the annual plan you’ll save around 30% compared to 12 months on the monthly plan.
What is Perlego?
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 1000+ topics, we’ve got you covered! Learn more here.
Do you support text-to-speech?
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more here.
Is Psychology of Eating an online PDF/ePUB?
Yes, you can access Psychology of Eating by Emily Crews Splane, Neil E. Rowland, Anaya Mitra in PDF and/or ePUB format, as well as other popular books in Psychologie & Psychopathologie. We have over one million books available in our catalogue for you to explore.
understand the relevance of diverse scientific disciplines to the psychology of eating
understand the derivation of body mass index and its relation to health and obesity
recognize the personal and society-wide economic burdens that are associated with problematic eating, including overweight or obesity and anorexia nervosa
recognize that both internal and environmental factors contribute to eating behavior
understand the internal sensations that produce eating or absence of eating
be able to discriminate reliable factual sources of information from “fake facts.”
We all engage in eating behavior, sometimes with pleasure or regret, but often just because it’s meal time. At its core, eating is a transaction, or rather several classes of transaction. The first transaction is between you, your body and its physiology, and the consumable item(s) in front of you. The second type of transaction is interpersonal, the bonds formed between you and the people with whom you are eating. For our hunter-gatherer ancestors, these were perhaps the main transactions, in part because the quality, safety, or security of the food could not be assured. A third type of transaction is recent in origin, but is now dominant, and that is the business aspect. In most countries today, food production, processing, and marketing are business propositions and food preparation is often performed by unknown agent(s) such as by retail sellers and restaurant personnel.
Commercialization of eating has brought with it a relentless tsunami of marketing and advertising about food products and a plethora of advice or information on what we should or should not eat, why we should eat a certain amount or way, and with what objective. As a result, eating has changed from a relatively simple act of sharing what the hunters or gatherers brought home on any given day, a world for which our prehistoric physiology was adapted, to a more complex situation in which eating is a series of decisions among competing media messages about food and/or the purpose or goals of that eating episode. Many of the food messages invoke underlying scientific (including medical) concepts yet the public has an imperfect understanding of those concepts and, as a result, is unable to evaluate information objectively and is susceptible to believing false claims or fake facts.
This introductory chapter has three principal aims. The first aim is to advocate that psychological science provides the integrative approach necessary to understand these complex transactional aspects of eating behavior. The second aim is to introduce some of the key terms or concepts related to eating and one of its consequences, body weight. The third aim is to start to discuss some guidelines or tools by which real facts might be discriminated from the fake facts that permeate mass media about eating.
Psychology: The Integrative Science
“You are what you eat” is a phrase that contains elements of truth yet conceals a more fundamental question of why you eat, with follow-up questions of what, where, when, and how much. If you think about eating as a scientific problem, it quickly becomes apparent that many disciplines are involved including psychology, neuroscience, biology, nutrition, economics, and more. A well-rounded approach to eating behavior must include each of these elements. Psychological science is an integrative discipline that is uniquely well positioned to bridge the streams of scientific thought that are relevant to eating and its problems (Figure 1.1). This text does not assume or require a substantial background in any specific discipline, but it does assume or imply a scientific approach.
FIGURE 1.1 Psychology occupies an interdisciplinary integrative role with regard to feeding behavior
Several books or monographs bear the title or subtitle “Psychology of Eating,” including those by Capaldi (1996), Logue (2015, 4th edition), Ogden (2010), and our first edition (Rowland & Splane, 2014), but we believe this text is the most integrative of the relevant science disciplines. Many other texts or monographs deal with the limited topic of eating disorders such as anorexia nervosa or bulimia nervosa. While these are serious and potentially fatal disorders, their incidence is an order of magnitude less than that of the conditions of overweight or obesity. These latter conditions, which together occur in almost 40% of adults worldwide and 70% in the USA, are seriously detrimental to health (Dahlgren, Wisting & Ro, 2018; Flegal et al., 2012; NDC Risk Factor Collaboration, 2016; Ogden et al., 2014).
From an historical or evolutionary perspective, it can be argued that the primary purpose of eating is (or was) to maintain an organism at a high level of physical strength in order to survive the rigors of life. This argument applies to both animals and humans and predicts, minimally, that eating should over time yield nutrients sufficient in quantity and quality to avoid weakness due to malnutrition and to support reproduction of the species. Societal advances in many domains – civilization in a broad sense – have greatly improved access to and quality of food. One result of that has been a much longer life expectancy and this has introduced a new purpose, namely the connection(s) between food, health, and longevity.
You are probably familiar with the term “unhealthy food” or its converse, healthy food. It is used in many messages, including media of all types, about food. But what does it mean? From a public health perspective, this concept might describe whether a food is contaminated with pathogens or poisons. Instead, common usage is a future projection that long-term consumption of that food carries a statistically higher probability of poorer health and/or shorter life span. That probabilistic inference also assumes abnormal or excessive consumption of the food. That is, “unhealthy food” is not an intrinsic property of the food: It is the behavioral interaction with that food that is unhealthy. It’s a case of what psychologists call external attribution: Blame an unwanted outcome on outside or environmental factors. When you next read, hear or are even tempted to use the adjective “unhealthy” or “healthy” in relation to food, stop and think about the assumptions behind that term! Several chapters in this book will address factors that influence this critical interaction between person and food.
Measuring Underweight, Overweight, and Obesity
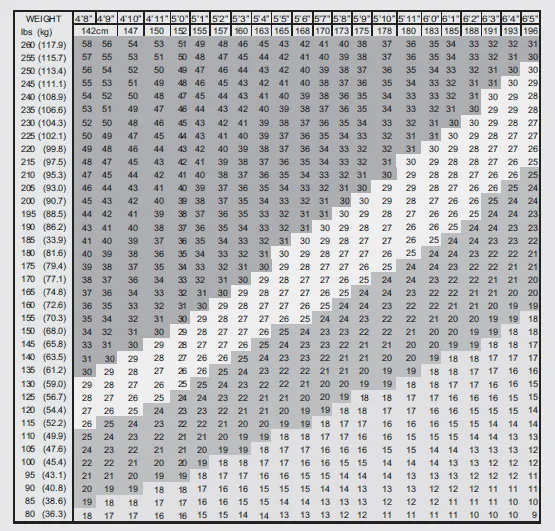
Earlier, we used the terms overweight and obese, and many of us have vaguely formed preconceptions about what they mean. In fact, they have a very precise scientific meaning that is based on pragmatic and simple biometric measurements of weight and height. Such measures are commonly made by medical or paramedical professionals, but can be made with reasonable accuracy by most people. Body mass index (BMI), a derivative metric, is body weight in kilograms divided by the square of height in meters (see Box 1.1 and Table 1.1). There are many published and online BMI calculators to make this easy. Ranges of BMI are widely used to categorize health and health outcomes. In particular:
BMI less than 18.5 = underweight
BMI 18.6–24.9 = normal or healthy
BMI 25–29.9 = overweight (also known as pre-obese)
BMI over 30 = obese (class I = 30–34.9, class II = 35–39.9, etc.).
TABLE 1.1 Body Mass Index Table
Source: body-mass-index-chart.gif
Note: Obese >30; overweight 25–30; normal 18.5–25; underweight <18.5.
After adolescence, an individual’s height does not change appreciably; thus, change in BMI of an adult most often reflects changes in body composition such as fat content. There is strong epidemiological evidence that elevated body fat content is associated with diseases such as hypertension, diabetes, osteoarthritis, and cancer (Wagner & Brath, 2012). High BMI often correlates with high body fat content although there are notable exceptions or limitations. For example, athletes in strength sports typically have elevated muscle mass, hence high BMI, but this does not reflect excessive fat. Further, BMI does not take into account potential gender, ethnic, or body frame differences. Excess fat in the central or abdominal region (more common in males) imparts increased risk of developing cardiovascular disease, whereas the same extra fat in the hips (more common in females) does not carry the same risk (Arsenault et al., 2012). A simple estimate of distribution of body fat is waist circumference and/or the ratio of waist to hip circumferences.
Box 1.1 How did BMI become a standard?
In 1943 the Metropolitan Life Insurance Company published actuarial tables of ideal weight for height for the purposes of calculating health risk and insurance premiums. American physiologist Ancel Keys argued vigorously about the inadequacies of these tables, and proposed instead the use of BMI (Keys et al., 1972). This index was not new at that time, but was devised in the mid-19th century by Belgian mathematician Antoine Quetelet in his use of anthropometric statistics to define “l’homme moyen” – the average man. Quetelet’s index, now called BMI, is weight (strictly, mass) divided by height squared. Mass refers to substance whereas weight depends on gravitational force but, since most of us live at one g, the terms are commonly used interchangeably in the field of health or nutrition. The universal measurement system of science is CGS (centimeter-gram-second) and BMI is expressed in CGS units for weight and height (viz., kg/m2). Use of other units (e.g., pounds and inches) requires a multiplicative constant to convert to CGS-based BMI values and is incorporated into most electronic BMI calculators.
Box 1.2 Do the Math
Imagine a 5ʹ2ʺ female starting college at 120 pounds. Over the next year she gains the mythical “freshman 15 (pounds).” Use an online calculator to compute BMI at the start and end of her first year. The next year, she gains an additional “sophomore 15.” What is the new BMI at the end of the second year? How do these BMIs map to weight categories? Her friend is a 6ʹ2ʺ male weighing 160 pounds at the start of his freshman year, and he has the same gain of 15 pounds each year. What are his BMI numbers and categories? (Answers are at the end of this chapter.)
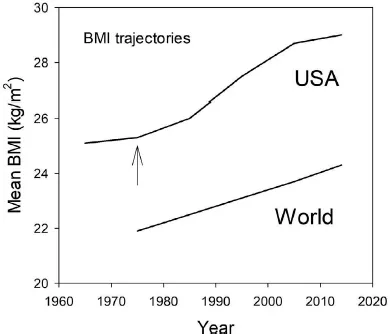
Using BMI as the index, overweight and obesity is a global problem. The World Health Organization (WHO) has compiled longitudinal data on BMI from over 19 million adults in 200 countries (www.who.int/gho/ncd/risk_factors/overweight/en/NDC; Risk Factor Collaboration 2016). Figure 1.2 shows one summary result from that report: The average BMI, shown as an average for men and women, rose from 21.9 to 24.3 kg/m2 between the years 1975 and 2014. This represents an increase of almost 3% per decade. Also shown in Figure 1.2 are BMI means for the USA dating from 1965, as published by the Centers for Disease Control (www.cdc.gov/obesity/data/prevalence-maps.html), summarized by Zimmerman (2011) and extrapolated by us from the WHO data. Perhaps not surprisingly, the WHO and CDC data show that Americans have a higher average BMI than the rest of the world, but the rate of increase since 1975 has been similar in most world regions and, from the USA data, there was a marked acceleration in this rate during the late 1970s (Box 1.3).
FIGURE 1.2 Mean body mass index (BMI) across time for the USA and for the world. Data are based on the WHO-NCD report (2016). The arrow shows the approximate onset of faster increase in the USA (data from Zimmerman, 2011)
Box 1.3 Marketing or Advertising?
Given the upward inflection in rate of change in BMI in the late 1970s, Zimmerman (2011) considered what underlying factors might have changed at about that time. In an affluent country like the USA, foo...