The focus on efficacy of the licenced practitioners’ actions in relation to individual patients came under scrutiny with the scientific developments of the Enlightenment. The philosophical move from logical deduction to inductive reasoning through the collection of empirical data began to change the emphasis from the actions of individual practitioners to systems-based understanding of health. As early as 1546, Girolamo Fracastoro proposed that disease was transmitted through the air and therefore should be controlled by personal and environmental hygiene in addition to specific individual patient treatments (Nutton 1990). Developing this theme, in 1847, Ignaz Semmelweis collected data to understand why mortality rates differed between two different maternity clinics in one city. In an early example of using the study of variation to understand practice and reveal underlying factors that are not immediately apparent, Semmelweis collected empirical data that demonstrated that clinics run by medical practitioners and their students had higher death rates than those run by midwives and their students. Semmelweis proposed that medical staff were inadvertently cross infecting women following their anatomy dissection sessions. He introduced hand washing between cases which dramatically reduced mortality rates (see Box 1.1).
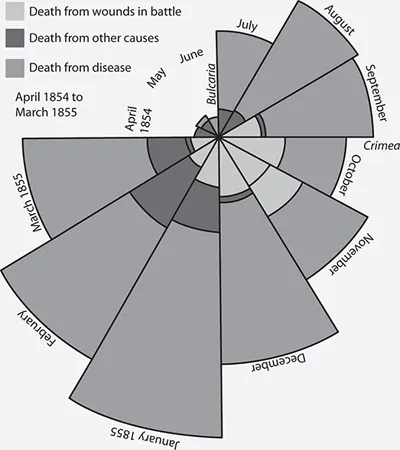
The central role of collecting data in understanding the causes of harm or quality failures was further demonstrated in 1854, when John Snow was able to demonstrate the importance of systems factors as well as individual patient factors when he methodically collected data about the location of the cholera cases (Shiode et al. 2015). Snow demonstrated that clusters of the disease were related to a contaminated water pump handle in Broad Street, London, and thus that environmental factors are as important as individual factors in improving health. Following quickly after this, Florence Nightingale (working with William Farr, Britain’s foremost statistician at the time) was able to show that soldiers were 10 times more likely to die from infectious illnesses such as typhus, typhoid, cholera and dysentery than from wounds acquired in battle (Nightingale 1858). Her creative use of data visualisation such as her coxcomb charts (see Figure 1.1) persuaded politicians to send the Sanitary Commission to the Crimea in March 1855. The resulting flushing of the sewers and improvement in the ventilation resulted in a sharp reduction in mortality rates. Florence Nightingale was honoured for her applied use of statistics by becoming the first woman elected to become a member of the Royal Statistical Society in 1858.
Box 1.1 Case study: Reducing the incidence of puerperal fever in Vienna
In the early 1840s, the people of Vienna widely believed that there was a significant difference in death rates between two maternity clinics, although they did not understand why this should be. In a rare example of patient involvement in quality improvement, Semmelweis collected patient opinions and described desperate women begging not to be admitted to one of the clinics, preferring to deliver in the street without any professional assistance. Semmelweis’s data suggested that even those who delivered without assistance had lower mortality rates than those who attended the other clinic, and he was puzzled that puerperal fever was rare among these women:
To me, it appeared logical that patients who experienced street births would become ill at least as frequently as those who delivered in the clinic. . . . What protected those who delivered outside the clinic from these destructive unknown endemic influences?
By collecting data on all deaths, Semmelweis uncovered a significant variation with one clinic having a maternal mortality rate of 10%, whilst the other clinic had a mortality rate that was significantly less at 4%. Having uncovered the variation, Semmelweis began to look at what the differences in practice between the two clinics were. The only major difference that he could ascertain was that the clinic with high mortality rates was used as a teaching clinic for medical students, whilst the other had been used exclusively for training midwives since 1841.
His realisation of this distinction was important. Changes to medical training meant that dissection had become an important part of teaching medical students anatomy during the 1800s but was not a part of midwifery training. Semmelweis began to consider whether there was some process associated with dissection that was the cause of the variation. Semmelweis knew that a medical student had recently died following a needle stick injury during a dissection and that his post-mortem had shown similar pathology to that of the women who were dying from puerperal fever. Whilst the pathology techniques available at the time could not empirically identify the causal factor, Semmelweis hypothesised that the (unknown) causal agent was somehow being transmitted from the corpses being dissected to the labouring women.
Although Semmelweis did not understand how dissection and puerperal fever were linked, he noted that there was a putrid smell associated with infected autopsy tissue that was removed by hand washing. To test this logic, Semmelweis undertook a period of observation and noted that at the first clinic, doctors and medical students routinely moved from dissecting corpses to examining women without first washing their hands. He proposed that the practice of hand washing with chlorinated lime solutions destroyed the causal ‘poisonous’ or contaminating ‘cadaveric’ agent at the same time as removing the smell.
Semmelweis collected data before and after his improvement and showed dramatic reductions in mortality after hand washing was introduced, with maternal mortality at the first clinic dropping from 10% to 1%.
Despite very clear data to support his improvement, Semmelweis’s observations conflicted with the established scientific and medical opinions of the time, and his ideas were rejected by the medical community. Semmelweis thus encountered the problem that persists today – evidence alone is not sufficient to sustain and spread even dramatic quality improvements.
Source: Semmelweis, I. The Cause, Concept, and Prophylaxis of Childbed Fever (translated by Carter, K., 1983), University of Wisconsin Press, London, 1861.