Preparation for endoscopy
Informed consent and counseling: The patient should be clearly informed about the procedure and the likely discomfort he may experience. It should be explained that his cooperation will make the procedure easier and quicker.
Overnight fasting: Routine endoscopy is usually performed in the morning hours after overnight fasting. Coating agents like antacids or colored medications should be clearly withheld. In case of obstructed stomach, prior nasogastric intubation and lavage should be performed to clear the gastric residue.
Sedation and anesthesia: For routine UGI endoscopy, we use only topical pharyngeal anesthetics such as lignocaine viscous or spray. Sedation, in the form of intravenous Midazolam, is occasionally used in children. For therapeutic endoscopy, such as foreign body removal, stent placement etc., it is our practice to use intravenous propofol anesthesia with or without endotracheal intubation.
Endotracheal intubation and monitoring: Endoscopy in a comatose or irritable patient is fraught with the risk of aspiration, hypoxia and “bite” damage to the endoscope. It is our practice to use prior endotracheal intubation and also monitor the vital parameters during the procedure.
Instrument check: Prior to endoscopy, it is good practice to check the instrument, including the light source, suction channel, airflow and display panel for any malfunction.
Position of the patient: Diagnostic endoscopy is always performed in the left lateral position. Occasionally, in a patient with upper GI bleeding, it may be necessary to examine the patient in the right lateral position. This is to displace the fundal blood pool that may obscure the bleeding lesion.
Antibiotic prophylaxis: Antibiotic prophylaxis is not indicated for diagnostic endoscopy. Current recommendations by the American Society for Gastrointestinal Endoscopy (ASGE) exclude even conditions such as valvular heart disease, prosthetic valves, synthetic vascular graft and prosthetic joints from the ambit of antibiotic prophylaxis. The few indications for antibiotic prophylaxis are therapeutic endoscopy for cirrhosis with acute variceal bleeding, cyst drainage and in patients with established GI tract infection who have the above listed cardiovascular status.
The mouth guard is held between the teeth. It is further supported by the index and middle finger of the endoscopy assistant. Alternatively, an elastic band attached to the mouth guard can be used to keep it steady.
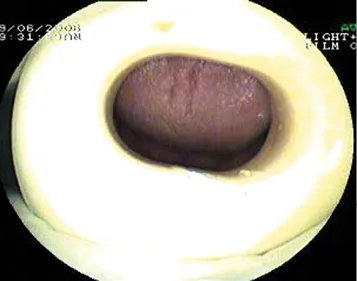
The tip of the endoscope is slightly bent to fit the contour of the tongue. It is gently advanced over the base of the tongue towards the pharynx.
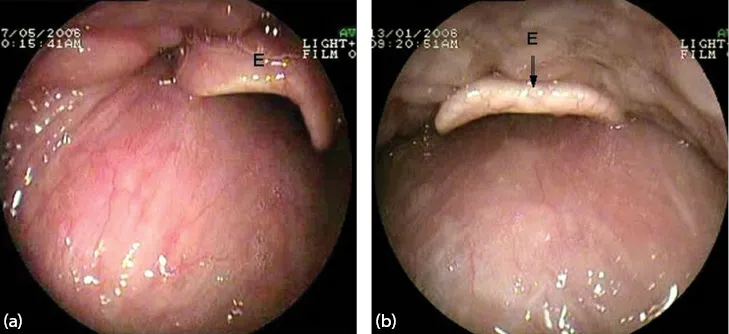
The epiglottis (E) is seen as the pharynx is entered.
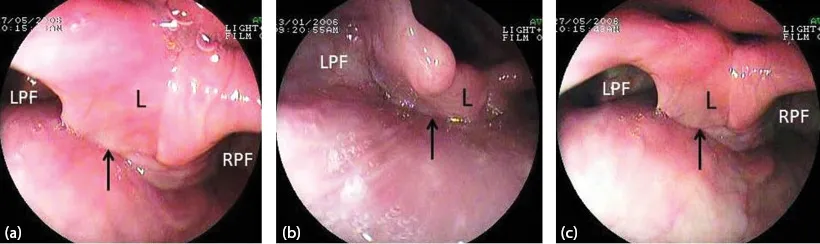
Figure 1.5 (a–c) The laryngo-pharynx. Larynx (L) and both pyriform fossae (RPF, LPF). The arrow points to the esophageal inlet.
As the scope passes below the epiglottis, the larynx and both pyrifo...