![]()
1 Introduction
In medical rehabilitation, there has been a long-standing tradition of collaboration between different professions and disciplines. Today, this work is often organized in teams, and there are good reasons for this. The most important reason is that teamwork has proven to give good results in terms of treatment outcomes. Another important reason is that teamwork is a form of organizing work that provides a sense of coherence to team members.
A classical text on teamwork in rehabilitation medicine (King et al. 1998) stated that much of the work which was previously mentioned via text is now a matter of eye-to-eye communication. Traditionally, healthcare systems have depended on written communication, with referrals, opinions, and prescriptions of various kinds sent back and forth between professionals, departments, and organizations, with the professionals involved in a patient’s care rarely meeting in person. Before teams were introduced, physicians in outpatient organizations worked primarily in solitude in their offices, physiotherapists were gathered in a specific part of the building, and medical social workers had their offices somewhere on the perimeter of the hospital. Unlike in inpatient wards, they never or very rarely met in person to discuss their respective interventions (with some obvious exceptions such as when performing a surgery). Of course, as everyone who works in the modern healthcare systems know, these conditions are changing in many places. It is becoming increasingly more common to organize the care around the patient and his or her needs, instead of around the historically understandable, yet progressively obsolete, organizations that saw the light in the post-WWII attempts at organizing hospitals in the same way as industries organized their production lines (Iedema 2007).
The distance between hospital-based care providers and other institutions such as community-based social services and job centers has been, and to a large extent still is, even greater. Numerous projects and reorganizations have been implemented to minimize the difficulties created by these divisions. Most of them seem to have failed. Others have succeeded as temporary projects, but, due to a lack of support needed to become a part of the ordinary organizational structure, they are seldom persisted with.
It is fair to say that the healthcare sector at large still wrestles with serious problems relating to communication and collaboration across borders of various kinds: between professions and disciplines as well as between organizational units such as clinics or across divisions between primary and secondary care (Iedema 2008). This does not mean that no such communication and collaboration takes place. It does. But the sub-optimized support for everyday communication and collaboration remains a problem in today’s healthcare systems, in spite of many attempts at improving the problems. According to the U.S. Agency for Healthcare Research and Quality, over 60% of all adverse events can be explained by deficit communication. However, it is important to note that it is normally not the individual care provider’s will to communicate and collaborate that is lacking, but rather the organizational will to allocate resources for developing procedures and protocols that do not swiftly return improvements in the balance sheet for the unit allocating the resources. The silo organization that characterizes most healthcare systems today simply does not support the kind of cross-boundary improvement projects necessary to improve this situation. And so, the enduring lack of dialogue between professions and disciplines continues to lead to sub-optimized solutions to problems that have not been understood in all their complexity—not because the people in the system do not understand that the problems are complex, but because the organizational support for collaborating and communicating across borders is lacking.
It is our experience that lack of well-developed collaboration and communication tends to increase feelings of meaninglessness, fatigue, and unnecessary antagonism in and between healthcare professionals. In the long run, it may also contribute to the growing numbers of long-term sick leave among healthcare personnel. When it comes to rehabilitation, several studies have shown that employers in rehabilitation teams with managers who support good teamwork have higher job satisfaction (Cartmill et al. 2010; Körner et al. 2010, 2015; Lundgren 2009).
This book is about teamwork within the field of rehabilitation medicine, which can in many ways be described as the discipline that first introduced qualified teamwork. Now, you may suggest that surgery surely was the first discipline to introduce teamwork, and in this you are partly right. But the purpose of this book is to present and discuss the kind of teamwork that is largely a matter of inventorying problems and possible solutions, reaching a shared understanding of both, and coordinating future actions. Teamwork in rehabilitation medicine is a way of overcoming the difficulties stemming from not communicating properly and in time about the problems the patient is facing and the possible solutions, and a way to adapt the care provided following the process of rehabilitation as it unfolds for the individual patient. Well-functioning teamwork in rehabilitation medicine can thus serve as an inspiration to clinical settings, where the key to delivering high-quality care is the need to understand the patient’s problems in all their physical, psychological, and social complexity, and being able to adapt the care provided in accordance with the individual patient’s needs, as they change over time.
The complicated and complex cases faced by those working in medical rehabilitation demand more dynamical and dialogical forms of collaboration than ever before. These days, the collaboration between different care providers does differ from the descriptions of King et al. cited earlier. An increasingly qualified and close cooperation between caregivers, patients, employers, social insurance offices, and/or insurance companies is becoming more and more common. Caregivers, not only in medical rehabilitation, do organize the care they provide across teams of various kinds. To solve complicated cases related to mental health issues or long-term pain, the efforts of highly qualified teams like those in rehabilitation medicine have proved to be a successful intervention. Qualified teamwork is beneficial not just for patients suffering from stress disorders or long-term pain that often cannot be cured by unimodal interventions; however, we explicitly mention these patients as they form a large part of the group who avail long-term sick leave in northern Europe. A large amount of the costs for society, as well as the suffering of individuals, is related to these problems. Other groups of patients also rely on rehabilitation professionals to recover from serious disease and trauma. Some of these groups have until quite recently not been provided with the rehabilitation care they need, which has left many with complex problems and functional deficits. Many affected persons are young and many stand a good chance to carry on with their lives normally if provided with proper rehabilitation. Some examples are survivors of stroke, traumatic brain injury, traumatic spinal injury, polytrauma, and cancer, including childhood cancer.
Even though we have come a long way, there is still a need for continuing development of the collaboration when it comes to these groups of patients. Much of the work related to these groups will be carried outside of the specialized rehabilitation clinics, predominantly in primary care and occupational care settings. Highly specialized rehabilitation clinics will only be involved in the most complicated cases. The majority of the workload will rest on primary care clinics and the occupational health services. Hence, this is where qualified collaboration involving not only various care-providing organizations but also care providers, the patient, and other involved parties such as employers, social security providers, and/or insurance companies must be developed. Another reason to emphasize these patients is that teams working with them meet a number of challenges that illustrate more general problems in teamwork, thus inviting more general discussions concerning medical rehabilitation and teamwork.
In the kind of qualified teamwork necessary to solve the type of problems mentioned above, the information the team needs to help a patient is gathered with the individual patient in focus. This means that the investigations carried out by each team member depart from a holistic perspective, where the actions taken by each team member are coordinated, goal-oriented, and individualized. But—and this is an important “but”—this type of organization takes an effort from every professional participating in it, as it requires not only a theoretical understanding of what a qualified teamwork is but also a willingness to change the ways in which one has worked before. When an organization commits to developing qualified teamwork, professionals who earlier hardly talked to each other except when they ran into each other in the corridors will now find themselves in meetings, face to face with colleagues from other professions and from other disciplines.
This book aims at showing how one can improve professional communication when discussing problems and solutions with colleagues who are not as familiar as one may want to think. It is based on our experiences within the Swedish healthcare system, where we have both worked with teams in a wide variety of clinical settings. Sweden is a society well known for its egalitarian and tolerant culture, and our understanding of what works and does not work in the realm of teamwork in medical rehabilitation is to some extent born out of our experiences in this context. We know that it is possible to prioritize information which may further the work of the team, regardless of where or who that information comes from. We also know that it pays off to endorse an atmosphere of active collaboration, active listening, and active dialogue. But this is not a book about how to become more Swedish. This is a book about the prerequisites for communication across borders of various kinds (professional, disciplinary, organizational) and the meetings that follow suit when teamwork is implemented in an organization. This book is about how to meet the demands that follow from implementing qualified teamwork, demands that have consequences for the professionals, the leaders, and the organizations in the healthcare system. This book is about teamwork in medical rehabilitation—the Swedish way.
REFERENCES
Cartmill C, Soklaridis S, Cassidy JD. Transdisciplinary teamwork: The experience of clinicians at a functional restoration program. Journal of Occupational Rehabilitation 21, 1–8, 2011.
Iedema, R. A. (ed.). The Discourse of Hospital Communication: Tracing Complexities in Contemporary Health Care Organisations. Basingstoke: Palgrave-MacMillan, 2007.
Iedema, R. A. Medicine and health, inter- and intraprofessional communication. In: Brown, K. (ed.), Encyclopedia of Language and Linguistics, 2nd edition, Amsterdam: Elsevier, 2008.
King JC, Nelson TR, Heye MI, Turturro TC, Titus MN. Prescriptions, referrals, order writing, and the rehabilitation team function. In: DeLisa JA, Gans BM. Rehabilitation Medicine: Principles and Practice. Philadelphia, PA: Lippincott-Raven Publishers, 1998.
Körner M. Interprofessional teamwork in medical rehabilitation: A comparison of multidisciplinary and interdisciplinary team approach. Clinical Rehabilitation 24, 745–755, 2010.
Körner M, Wirtz MA, Bengel J, Göritz AS. Relationship of organizational culture, teamwork and job satisfaction in interprofessional teams. BMC Health Services Research 15, 243, 2015.
Lundgren, C. Samarbete genom samtal: en samtalsanalytisk studie av multiprofessionaella teamkonferenser inom smärtrehabilitering [Collaboration and Conversation: A Discourse Analytical Study of Multiprofessional Team Conferences in Pain Rehabilitation]. Linköping: Linköping Studies in Arts and Science, 483, 2009.
![]()
2 Historical background
This chapter is concerned with how the organization of vocational work with relevance for teamwork has changed over the past century. We give a brief historical overview of teamwork’s deep roots in industrial management and show how these roots influence team-based organizations today.
ORGANIZATION THEORY AND ORGANIZATIONAL CHANGE
The rapid growth of teams as a way of organizing work in healthcare must be understood against the backdrop of theories and trends in organization management at large. These trends, stemming from the industrial production of goods as well as the production of services, have played, and still play, an important role in the development and organization of the healthcare sector. Classical industrial organization theory is useful when trying to solve some problems in the healthcare sector, but, as we shall see, far from all.
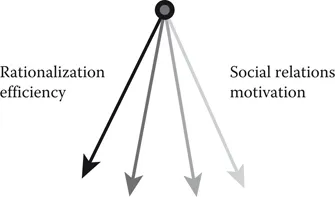
Even though the human body is to some extent standardized and some aspects of human life, illness included, can benefit from being treated in an equally standardized way, the individual human is more than the sum of its physical components. Humans are complex and adaptive, and entangled in contexts of relations with other humans. This means that no patient can be treated like any other patient, in spite of the fact that they may suffer from the same illness. Despite the attempts at streamlining the healthcare sector, the hallmark of healthcare remains to be that many tasks are extremely shifting and complex, thereby requiring tailor-made solutions offered by highly skilled, flexible professionals. This is, and always will be, quite far from tasks in the traditionally organized work in the production industry sector, which is typically characterized by predictability, standardization, and repetition, to such an extent that parts of it can be carried out by robots. The healthcare sector deals with complex, adaptive, individual human beings. When trying to grasp some of the major themes in organization theory during the past century, it soon becomes obvious that the pendulum swings back and forth between two opposite pools (Brulin and Nilsson 1997). One of the pools is the focus on issues such as rationalization and efficiency, issues connected with the type of problems that can be governed by managers at various levels in an organization. The other pool is the focus on the human and relational perspective, on the everyday life of the employees, and on issues such as social relations and motivation.
In this chapter, we have chosen to highlight four themes that are central to the understanding of teams as a way of organizing work: Taylorism, self-management groups, quality management, and, finally, the emergence of teamwork.
Taylorism
The first swing of our imagined pendulum, toward the side of efficiency and productivity management, originates from the thinking of American engineer Frederick W. Taylor (1856–1915). Taylor’s ideas about industrial production gained momentum during the industrial revolution in the beginning of the 20th century and are commonly referred to as Taylorism or scientific management (Kanigel 1997) (Figure 2.1). During this time, craft work was transformed via mechanization into industrialized manufacturing. Taylor and his peers did not foresee humans being exchanged for automated systems and robots, as he obviously felt that humans would be the agents of mechanized manufacturing. In his time, the focus on implementing production line principles was nothing but a revolution.
A very important idea in Taylor’s philosophy is that it is the management and not those in production who have the necessary overview to plan production. Another central point in Taylor’s philosophy is that it is possible for an expert to identify one best and rational way of solving every task. This rationalistic view on manufacturing had a very strong impact not only in the United States but also in Europe. A third central point of Taylor’s thinking is that the individual worker must be easily replaceable. The underlying logic of Taylorism is to lessen the importance of the individual worker, via the processes of knowledge transfer and division of work, thus minimizing the risk of efficiency losses connected to dependence on highly skilled workers.
Figure 2.1 During the 20th century, the pendulum has swung back and forth between the rationalistic and the relational pools several times.
This idea about organization is difficult to apply to the extremely complex and knowledge-intensive organizations in healthcare. However, the principle of interchangeability is vital in 24/7 care s...