This easy yet comprehensive reference guide covers the mechanisms of respiratory diseases, explaining the main respiratory conditions for clinicians and postgraduate trainees. It discusses their aetiology as well as the basic concepts required to effectively evaluate and treat them. Applied Respiratory Pathophysiology is the first book to bring together detailed, clinically-relevant explanation of respiratory physiological processes and pathophysiological processes in one text. It is essential reading for anyone diagnosing and treating specific clinical conditions of the lungs.
- 292 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Applied Respiratory Pathophysiology
About this book
Information
1
Embryology, anatomy, and histology of the lung
Introduction
Embryology
Embryonal stage
Pseudoglandular stage
Canalicular stage
Saccular stage
Alveolar stage
Anatomy and histology
Conducting airways
Exchange surfaces
Vasculature
Lymphatic drainage
Innervation
Ultrastructure
References
Introduction
The respiratory system allows gas exchanges between ambient air and blood circulation by extracting oxygen from inhaled air into blood and rejecting carbon dioxide from the blood into exhaled air. This function is accomplished by the interplay of the three functional components of the respiratory system: conducting airways, exchange surfaces, and a ventilatory apparatus (Figure 1.1).
Conducting airways do not simply conduct air between the external environment and the exchange surfaces. They also humidify and warm inhaled air, and eliminate inhaled dusts and microorganisms. Upper airways include the nasal cavity, nasal sinuses, nasopharynx, oropharynx, and larynx. Lower airways extend from the trachea to the bronchi and their successive ramifications down to terminal bronchioles. Exchange surfaces are specialized in the rapid gas exchange between inhaled air and blood circulation. They are made of respiratory bronchioles, alveolar ducts, alveolar sacs, and alveoli. The ventilatory apparatus includes bones and muscles of the thoracic cage, diaphragm, and abdomen as well as elastic tissues from the pleura and the lungs, and finally respiratory centers in the brainstem and afferent/efferent nerves. Approximately 10–12 times per minute, the brainstem sends an automatic inspiratory signal to the diaphragm via the phrenic nerves and to other muscles of the thoracic cage. Their contraction causes an expansion of the thoracic cage and lungs, which drives external air containing 21% oxygen and less than 1% carbon dioxide into airways, down to the exchange surfaces. Then, the inspiratory signal ceases and the thoracic cage passively returns to its resting position. In doing so, the inhaled air, now containing only 16% of oxygen and 6% of carbon dioxide, is then exhaled. This chapter describes the embryology, anatomy, and histology of the respiratory system. It is based on major reference textbooks on the subject [1–6].
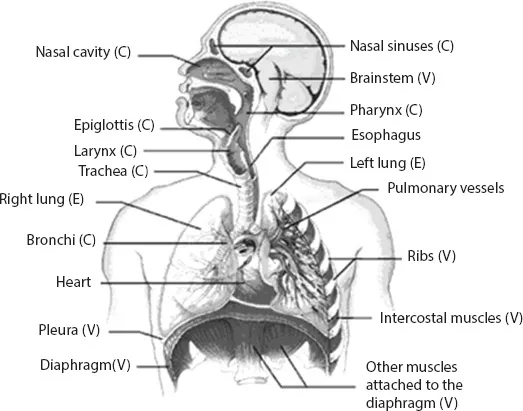
Figure 1.1Anatomic structures of the respiratory system. Function indicated in parentheses: conducting airways (C), exchange surfaces (E), and ventilatory apparatus (V).
Embryology
The lungs do not perform a respiratory function during intrauterine life. Instead, they are responsible for the production of amniotic fluid. Lung development is classically divided into five stages, which partially overlap one another and correspond to the successive establishment of conducting airways, transition airways (respiratory bronchioles), and exchange surfaces. This process results in an average of 16 successive dichotomic ramifications of the conducting airways, and in seven additional levels in the transition airways and exchange surfaces, resulting in a total of about 23 levels of ramification from the trachea to the alveoli. Extrauterine life is only possible from the 24th week of gestation, when a functional pulmonary vasculature appears and the production of surfactant begins. Figure 1.2 summarizes the development of the respiratory system.
Embryonal stage
At days 26–28 after conception, two pulmonary buds form at the distal extremity of the laryngotracheal groove on the ventral pharynx. They will become the right and left mainstem bronchi. The right bronchial bud is oriented vertically whereas the left bronchial bud is almost horizontal. Bronchial buds also subdivide inequally into three lobar bronchi on the right side and only two on the left side. The pulmonary asymmetry of adult age is thus established early in the development. At the end of the embryonal stage, all the segmental bronchi of the pulmonary lobes are formed.
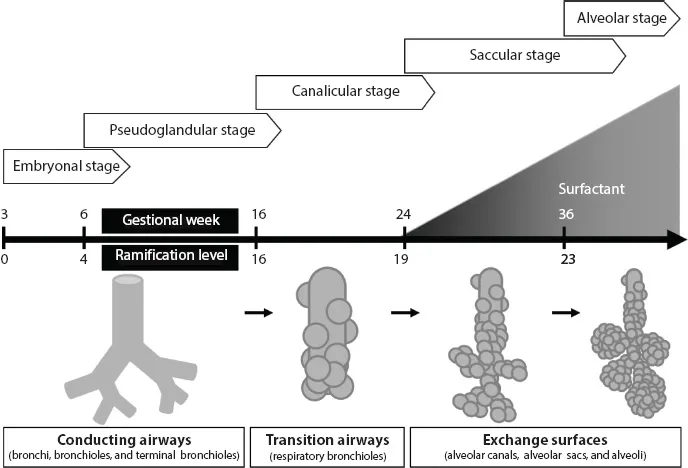
Figure 1.2Development of the respiratory system. Embryonal and pseudoglandular stages are marked by the establishment of conducting airways. Canalicular stage is characterized by the formation of respiratory bronchioles, a transition between conducting airways and exchange surfaces. During saccular and alveolar stages, the first exchange surfaces develop and surfactant production starts, marking the beginning of a potential for extrauterine fetal viability. At the 36th week of gestation, a definitive ramification level of 23 is reached from the trachea to respiratory bronchioles but alveolar acquisition continues after birth and until the age of 8 years.
Pseudoglandular stage
From the 6th to the 16th gestational weeks, the entire conducting airways are formed by a succession of ramifications culminating in the terminal bronchioles. These ramifications are under the control of the primitive mesenchymal tissue surrounding the airways in which proliferation genes are activated at the ramification points. This primitive mesenchymal tissue will later differentiate into bronchial cartilage, blood vessels, smooth muscle, and connective tissue.
Canalicular stage
From weeks 16 to 26, canalicules originating from the terminal bronchioles begin to constitute the pulmonary parenchyma. All respiratory units derived from a specific terminal bronchiole form an acinus, which includes 3–4 generations of respiratory bronchioles, extended by alveolar ducts that then bud into alveolar sacs. The milestone of canalicular stage is the modification of both the primitive mesenchymal tissue and the epithelial lining into a conformation allowing a potential for respiratory function. Specifically, along all terminal bronchioles and other structures derived from them, the primitive mesenchyma develops as a delicate network of capillaries that brings the blood circulation into intimate contact with exchange surfaces. Also, the lumen of the canalicules, and later of their derivatives, enlarges while part of their epithelial lining flattens, thin (squamous) type I pneumocytes differentiating from cubic type II pneumocytes. At the end of canalicular stage and the beginning of saccular stage, type II pneumocytes also begin to secrete pulmonary surfactant (surface acting agent). The chemical composition of this substance (mainly glycerophospholipids, proteins, neutral fats, and cholesterol) prevents alveolar collapse during expiration from birth and thereafter by reducing the surface tension of the alveolar surfaces it covers. These changes are pivotal as they mark the beginning of a potential for extrauterine viability for the fetus around the 24th week of gestation. Pulmonary maturation can be measured by the ratio between surfactant lecithin and amniotic fluid sphingomyelin, with the lecithin/sphingomyelin ratio increasing as the lungs mature. The administration of steroids can accelerate pulmonary maturation and surfactant production in premature neonates.
Saccular stage
Between 24 and 38 weeks of gestation, additional exchange surfaces are generated by alveolar sacs forming at the end of alveolar ducts, hence the name saccular.
Alveolar stage
During the last weeks of pregnancy, new alveolar sacs continue to form, eventually leading to their final and smallest subdivisions, the alveoli. This “alveolarization,” or alveolar development, continues massively during the first 6 months after birth, and to a lesser extent until the age of 8 years, after which the alveolar count culminates at 300 millions. In adulthood, the total alveolar surface is estimated to reach 80 m2, the equivalent of a badminton court.
Anatomy and histology
Conducting airways
Airways not only do “conduct” but also “clean,” warm, and humidify inhaled air. Hairs at the very entrance of upper airways in the nasal vestibule filter du...
Table of contents
- Cover
- Half Title Page
- Title Page
- Copyright Page
- Contents
- Preface
- Acknowledgments
- Contributors
- 1 Embryology, anatomy, and histology of the lung
- 2 Physiology of the respiratory system
- 3 Laboratory techniques to study the cellular and molecular processes of disorders
- 4 Acute respiratory insufficiency
- 5 Pathophysiology of asthma
- 6 Chronic obstructive pulmonary disease
- 7 Pulmonary vascular diseases
- 8 Respiratory infections
- 9 Sleep-related breathing disorders
- 10 Interstitial lung diseases
- 11 Lung cancer
- 12 Occupational respiratory diseases
- 13 Diseases of the pleura
- 14 Cystic fibrosis (mucoviscidosis)
- 15 Bronchiectasis
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Applied Respiratory Pathophysiology by Louis-Philippe Boulet in PDF and/or ePUB format, as well as other popular books in Medicine & Clinical Medicine. We have over 1.5 million books available in our catalogue for you to explore.