Pain and Its Relief Without Addiction will help people in pain understand why their pain is not always adequately relieved, as well as help reverse the failure of current medical practice to routinely alleviate pain. As noted by a 1992 publication of the United States Department of Health Services, this devastating trend contributes to unnecessary discomfort, longer recovery periods, and compromised patient outcomes. By reading this book, frustrated physicians and, perhaps more importantly, persons in pain can acquire a better understanding of the nature of pain, its connection to the emotions and psychological state of patients, and the impact particular drugs have on the body; this will facilitate relief from pain among a higher percentage of the population.Opioid analgesics comprise many of the chapters in Pain and Its Relief Without Addiction. Author Barry Stimmel, MD, describes the principles to be followed in prescribing opioid analgesics to relieve pain while maintaining one's daily activities without any limitation in function. The available opioids are described, and the differences between them are reviewed to allow you--as a physician, health care provider, or even a patient--to gain a better insight into the one(s) to use for both acute and chronic pain states. The point that is emphasized is that dependency on an analgesic to relieve pain is no different than dependency on medications to lower blood pressure, prevent heart attacks, treat diabetes, etc. What should be avoided is "addiction," a condition where function is impaired rather than enhanced.Pain and Its Relief Without Addiction is a guidebook designed to assist physicians and other health professionals in developing a practical approach to pain management and to give patients a fuller understanding of their pain. You'll gain specific information about:
- management of acute and chronic pain
- pain in children
- pain and cancer
- pain and AIDS
- psychological support of persons in pain
- theories of pain perception
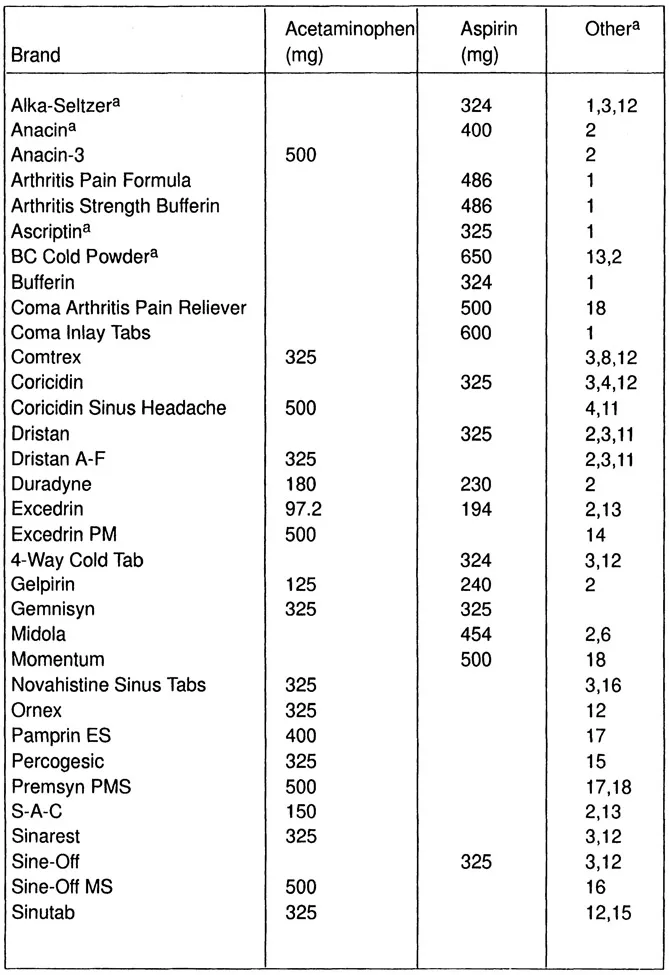
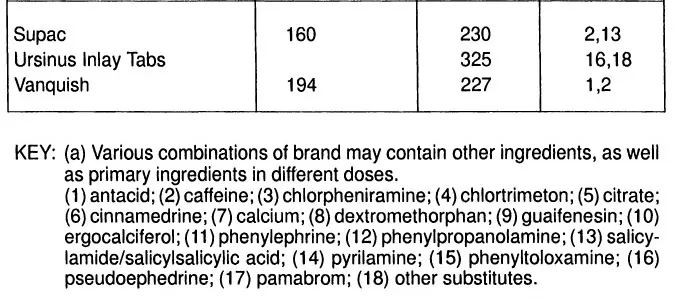
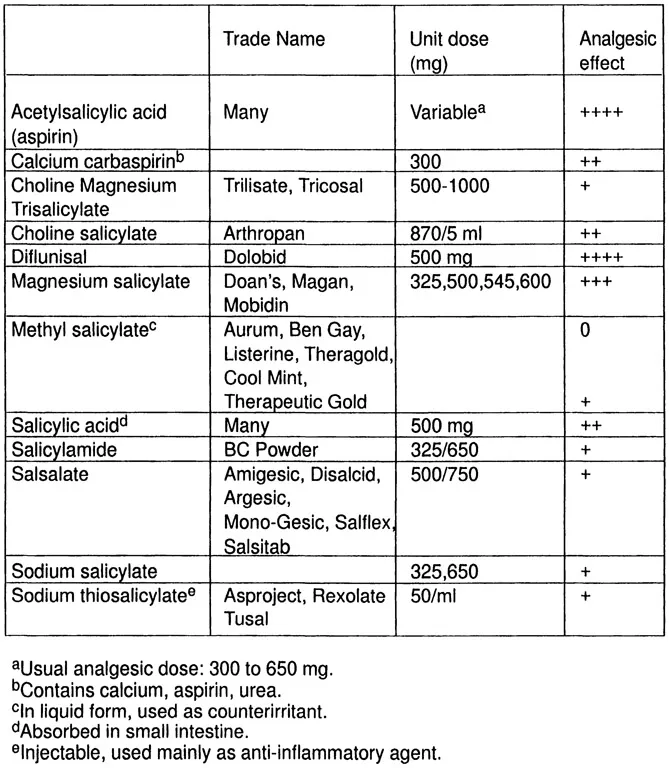
- the anatomy of painIn Pain and Its Relief Without Addiction, you'll learn the basic concepts of drug dependence, tolerance, and withdrawal, the pharmacological actions and side effects of drugs used to provide analgesia, and the fundamental steps to be taken in proper pharmacological treatment of pain. The book produces more effective and more informed communication among physicians, other health professionals, and patients so that together they can achieve better pain relief. As Pain and Its Relief Without Addiction illustrates, it is crucial that both patients and physicians understand clearly the terms describing drug use and the behavioral, biochemical, and cellular concepts underlying dependence, tolerance, and withdrawal. Finally, you will acquire a knowledge of all the potential causes of pain and the appropriate steps for intervention.Medical students, new practitioners, and those wishing to reconsider their approaches to pain management will benefit from the book's coverage of general principles for pain control, the use of drug combinations to provide the most effective relief, methods for treating pain in different populations (such as the elderly and persons with chronic medical conditions), and alternative options for failed treatment. The scope of Pain and Its Relief Without Addiction reaches from nonprescription medications, such as aspirin, to NSAIDS, like ibuprofen, to narcotic analgesics to stimulants such as amphetamines and caffeine. It is the most comprehensive book available on various drugs, their desired effects and side effects, and their use to alleviate pain.