eBook - ePub
The New Injection Treatment For Impotence
Medical And Psychological Aspects
- 220 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The New Injection Treatment For Impotence
Medical And Psychological Aspects
About this book
In this volume, two experts on sexual disorders describe the most effective treatment yet developed for male impotence. The authors review both the medical and the psychiatric aspects of injection treatment for men of all ages, with particular attention to older men and those with psychogenic impotence. The authors also discuss ethical considerations.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
History & Theory in PsychologyIndex
PsychologyCHAPTER I
____________
Historical Perspectives
____________
A. The History of Modern Sexology
RECENT DECADES have witnessed dramatic advances in our understanding of the mechanisms of erection and in our ability to treat impotence. Until very recently, remarkably litde was known about the physiology of the human sexual response or about sexual pathology. Thus, in the sixties our concepts about the etiology of sexual disorders were still completely erroneous and treatment was so ineffective that many patients who suffer from what we now think of as minor erection difficulties were doomed to a lifetime of chronic impotence.
This appalling situation did not come about because sexuality is especially complicated. In fact, sexology is basically much simpler than, for example, neurology or cardiology, which were far more advanced. But sexual medicine lagged far behind the rest of medicine because the puritanical attitudes prevailing in our society until the advent of the “sexual revolution” had made the scientific study of human sexuality impossible until just a few years ago.
Actually, interest in the treatment of impotence dates back to the very beginnings of medicine. Pre-Christian societies were unabashedly interested in sex and placed great importance on sexual adequacy. Thus, it is not surprising that the writings of such distinguished Greco-Roman physicians and philosophers as Hippocrates, Lucretius and Pliny the Elder contain extensive discussions of remedies for impotence and infertility.
Despite this promising beginning, because of the singular moralistic significance ascribed to human sexual behavior in the Judeo-Christian dogma, sexology was the last of the biological disciplines to cast off the shackles that had hampered medical research in the Western world for some two thousand years. And so, while the other specialities were rapidly advancing into the nuclear age, sexual medicine had, until recently, remained in the dark ages.*
Today, the situation is completely different. Thanks to the amazing progress made since the scientific study of human sexuality became socially acceptable during the forties, we now have a clear understanding of the human sexual response and of the pathogenesis of sexual disorders. As a result, the modern multidisciplinary approach to the treatment of sexual disorders has become so effective that we can now help the majority of patients with potency problems.
THE SCIENTIFIC STUDY OF SEX
The Pioneering Work of Masters and Johnson
The first significant breakthrough that ushered in the modern era of clinical sexology was made by William H. Masters and Virginia E. Johnson. Their great contribution actually consisted of a rather simple study, but one that would have been unthinkable in the old antisexual days. With scientific objectivity, these two courageous scientists painstakingly observed and recorded 14,000 separate human sexual acts. In their laboratory, behind a one-way mirror, they watched men and women masturbate, engage in intercourse in various positions, have oral sex, have anal sex, have sex while the woman was menstruating, and so on.
Masters and Johnson documented the human sexual response with the help of special recording devices. For example, they developed a method for attaching electrodes to, and recording the muscle activity of, the genitalia during intercourse. They built a camera into a translucent plastic phallus and used this to record vaginal responses during sexual stimulation. In their landmark book, The Human Sexual Response, which was published in 1966, Masters and Johnson finally gave the world a carefully documented, accurate, scientific description of the physiology of the male and the female sex organs.
But this descriptive analysis of genital functioning, although extremely useful, was only a first step. The next great breakthrough was the reconceptualization of the outdated monistic view of human sexuality. A new triphasic paradigm corrected some of the old erroneous views of sexual physiology and of the pathogenesis of sexual disorders, while also incorporating the motivational aspects of sex into the model of human sexuality (Kaplan, 1977, 1979).
The Triphasic Concept of Human Sexuality and the Sexual Disorders
Since the beginning of time, the human sexual response had been considered to be a single physiological entity, commencing with arousal, developing into excitement, and ending in a climax. This was a major error that gave rise to another serious misconception: that all sexual disorders were variants of a single clinical entity that was labeled “impotence” in men and “frigidity” in women.
We now know that in actual fact the human sexual response of males and females is composed of three related, but neurophysiologically and anatomically distinct phases: sexual desire, sexual excitement and orgasm, and we have learned that there are a number of different, clinically distinct sexual disorders that require different treatment approaches.
The first step in dispelling the myth that all sexual disorders were simply forms of impotence or frigidity was made by James Semans, a urologist, before Masters and Johnson’s work was published. In a short paper, Semans described the successful treatment of eight premature ejaculators by a procedure now known as the “stop-start” method of interrupted penile stimulation (Semans, 1956). Prior to Semans’ astute clinical observations, premature ejaculation (PE) had been classified and treated (unsuccessfully) as a form of impotence, which was then termed “ejaculatory impotence.”
The true significance of Semans’ discovery was not realized for a long time. But in retrospect we now know that apart from inventing an ingenious method for treating PE, which is still, with some modifications, used today (Kaplan, 1989a), Semans was the first to distinguish between erectile failure or impotence, and PE, which is a failure of ejaculatory control but does not involve erection difficulties.*
The last chapter in the evolution of the modern concept of sexual disorders came in the late seventies as a result of reviewing our treatment failures. By then, we had advanced to a “biphasic” view of sexuality, which recognized the clinical distinction between and the different treatment requirements of erectile and ejaculatory disorders; sex therapy had been developed to a point where it was so effective that any treatment failure warranted a closer look. The analysis of our failures led to the realization that some male patients who had complained of impotence had not improved because we had made an error in our assessment. We had treated these patients with our standard sex therapy protocol for impotence because we had not recognized that their complaints of erectile failure had been secondary to their diminished sexual interest, and that they were actually suffering from low (hypoactive) sexual desire** (Kaplan, 1977, 1979). These patients had attempted to make love to their wives out of a sense of duty although they felt little desire. Not surprisingly, they had developed problems in attaining and maintaining their erections.
One reason for our oversight was that these men had found it less threatening to their partners to complain about their own performance problems than to admit to having lost their sexual interest in their partners. In our desire to support the couples’ relationships, we had “bought into” their denial. Once we became aware of this, we found that the complaints of many of our impotent patients centered around dissatisfaction with the subjective aspects of sex—lust or desire.
We now know that desire is an important aspect of human sexuality and that inhibited sexual desire is a distinct psychosexual disorder. Moreover, patients with deficient sexual desire have a poor response to sex therapy methods that are designed for treating psychogenic impotence, although they do well with other forms of sex therapy.
The separation of the sexual disorders into the different phase-related syndromes has had significant clinical implications.* The triphasic system of classification provides the theoretical basis for understanding the distinctive clinical features as well as the pathogenesis of impotence, as distinct from sexual problems of desire or ejaculation. Ultimately, these insights have led to the development of specific and more effective treatments for impotence, as well as for the other sexual disorders.
TABLE I.1
The Three Phases of the Male Sexual Response Cycle
The Three Phases of the Male Sexual Response Cycle
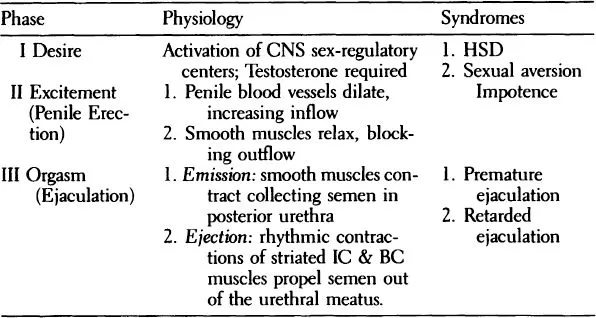
According to the triphasic concept of Human Sexuality (Table I.1) the sexual response of males (and females) is composed of: one, sexual desire, which represents the subjective experience of lust that accompanies the activation of the sex regulatory centers in the limbic brain; two, sexual excitement, which is a local vasocongestive response that changes the male genitalia from their quiescent state to the erect reproductive phallus; and three, the orgasm phase, which in males consists of two subphases—emission and ejection, which are produced by the reflexive contractions of smooth and striated genital muscles respectively.
THE CLINICAL FEATURES OF THE MALE SEXUAL DISORDERS
Under nonpathological circumstances, sexual desire, excitement, and orgasm overlap in time. This, along with the synchrony that normally exists between the three phases of the sexual response cycle, makes it appear as a single, smooth sequence. But the essential biological discreteness of libido, erection, and ejaculation is clearly revealed in pathological states. For the male, sexual response is seldom destroyed completely, either by organic disease or by psychological stressors. In clinical practice, we typically see the impairment of one of the three phases, while the others are spared. The clinical features of the various sexual dysfunction syndromes are the results of this phase-specific pattern of impairment (Kaplan, 1977, 1979). (See Table I.1)
The chief clinical feature of impotence is the failure to attain or maintain an erection firm enough for vaginal intercourse. However, impotent men often retain their interest in sex and many can experience pleasurable ejaculations although their penis remains flaccid. It is only the erectile or vasocongestive excitement phase of the sexual response cycle that is impaired in impotence.
On the other hand, men with retarded or premature ejaculation (RE or PE) generally have normal sexual desire and, unless they develop secondary impotence, have no erectile difficulties. These patients suffer from overcontrol of the ejaculatory reflex, which is the chief clinical feature of retarded ejaculation, or from inadequate control, which characterizes premature ejaculation.
Men with hypoactive sexual desire have no primary potency or ejaculatory disorders. The diagnostic criterion for HSD is a lack of sexual desire, which may be global or confined to the partner. Unless secondary impotence complicates the clinical picture, these patients are capable of having intercourse, albeit mechanically and without much pleasure.
The different sexual syndromes are produced by different sets of causes and they respond to different treatment strategies. The clinical significance of this concept extends to ICI, in that this is an appropriate treatment modality only for erectile difficulties and should be used exclusively to treat impotence. This therapy is of questionable value, and in some cases is potentially harmful for patients with ejaculatory and desire phase sexual disorders.
SEX THERAPY
Before Masters and Johnson published their groundbreaking volume, “Human Sexual Inadequacy” (1970), it was believed that psychosexual disorders are always the product of severe unconscious neurotic sexual conflicts that originate in serious childhood trauma. In accordance with this theory, lengthy and costly psychoanalytic treatment was recommended for every impotent patient. But the results were extremely poor.
Masters and Johnson made their second immensely important contribution by demonstrating that the psychoanalytic formulation of psychosexual symptoms was not necessarily valid in all cases and that extensive insight therapy was not the best treatment for the majority of patients with sexual dysfunctions. They found that in many cases psychogenic sexual disabilities are the product of less complex and more consciously recognized causes, such as the simple fear of not being able to perform sexually.
Moreover, they demonstrated that long-standing sexual problems, such as impotence and PE, could often be cured rapidly, in two weeks, with their highly innovative cognitive—behavioral, couples oriented therapy program, which stresses the reduction of performance anxiety and improvement of the partners’ communications. Masters and Johnson published the results of their remarkably successful rapid treatment program in 1970, and some people thought this spelled the end of psychoanalysis.
But this did not happen. It turned out that a significant proportion of sexually dysfunctional individuals, as well as their partners, are resistant to the rapid behavioral modification of their sexual symptoms because of their concurrent deeper emotional, sexual, and/or marital conflicts. Thus, in the seventies, in order to meet the challenge of the resistant patient, a new sex therapy approach was developed that combines the behavioral modification of sexual symptoms of classic sex therapy with brief, active, psychodynamically oriented management of the patient’s resistances (Kaplan, 1974a). This integrated approach, called “The New Sex Therapy,” has been widely accepted.
The New Sex Therapy
Brief, psychodynamically oriented sex therapy employs structured erotic interactions that the couple or patient carry out in the privacy of their home. These therapeutic behavioral interventions, which include but are not limite...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Dedication
- Table of Contents
- Preface
- Chapter I. Historical Perspectives
- Chapter II. Erection and Impotence
- Chapter III. Pharmacology
- Chapter IV. Diagnosis
- Chapter V. Injection Therapy for Impotence
- Chapter VI. The Psychiatric Aspects of Injection Treatment
- Chapter VII. Injection Treatment for Older Patients
- Chapter VIII. Injection Therapy for Psychogenic Impotence
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The New Injection Treatment For Impotence by Gorm Wagner,Helen Singer Kaplan in PDF and/or ePUB format, as well as other popular books in Psychology & History & Theory in Psychology. We have over 1.5 million books available in our catalogue for you to explore.