1
Worldwide Innovations in Health Insurance Reform
X. Scheil-Adlung
In most countries today social health insurance forms an important part of daily life for the population and is regarded as extremely important. However, systems that have developed gradually over many years now find themselves confronted by clearly defined limits. There are still population sectors excluded from social protection without equal access to health insurance. Severe funding problems and cost increases set limits on possibilities for reform and population ageing is leading to new pressures on costs.
• How can adequate health care be provided for as many people as possible at reasonable contributions and cost?
• How can funding shortfalls, over- and under-provision of care, waste and administrative inefficiency in social health insurance systems be prevented?
• How can health care institutions be organized in a more future-oriented way?
• What solutions are there to such structural problems for health insurance systems with population ageing and its concomitant upward pressure on costs?
Both industrialized and developing countries have been working intensively for several years on answers to these central questions for social health insurance systems.
How can adequate health care be provided for as many people as possible at a reasonable cost?
The search for solutions with regard to more equal access to health care involves both the formal and informal sectors of the economy. Efforts are aimed in particular at social health insurance for salaried workers, the self-employed, immigrants, asylum seekers, illegal workers, domestic and agricultural workers, and family dependents.
How can funding shortfalls, over- and under-provision of care, waste and administrative inefficiency in social health care systems be prevented?
Most countries are being forced to look for new, socially acceptable solutions as a result of rising financial pressure on state budgets and rising health costs.
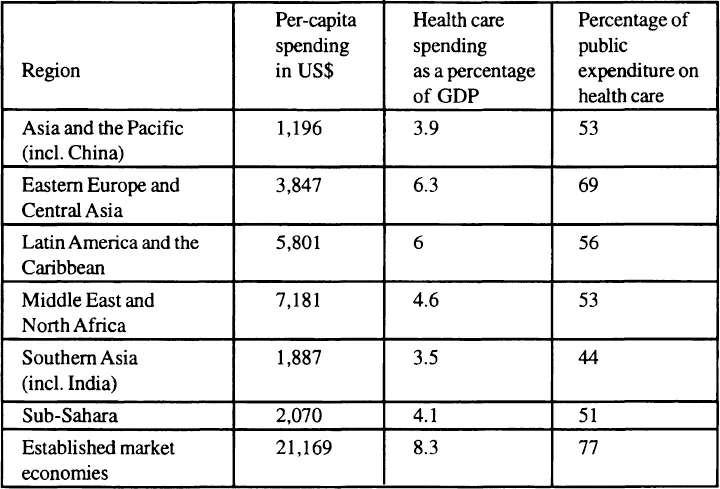
Table 1.1
Health Care Spending by Region, 1994
Source: Adapted from G. Schieber; A. Maeda. 1997. “A Curmudgeon’s guide to financing health care in developing countries,” World Bank, An International Conference, Innovations in health care financing” Washington D.C., March 10–11.
• In statistical terms1 the 1994 figures for per-capita expenditure on health varied from US$1,196 in Southeast Asia and the Pacific and up to US$21,169 in established market economies. For the same period health spending as a percentage of GDP varied from less than 4 percent (Southeast Asia and the Pacific) to over 8 percent (established market economies). The public share of health spending varied from 44 percent (Southeast Asia including India) to 77 percent (established market economies) as table 1.1 shows.
On the one hand financial pressures lead to the search for new funding sources and methods, while on the other the possibilities for rationalization have largely been exhausted. Efforts are now being directed at removing over- and under-provision of health care and administrative inefficiency and using new information technology to provide better services.
The pressures of costs, however, are also leading to a situation where a delicate balance between the affordable, and the socially desirable has to be found and defended politically. Each decision is of great ethical importance. In the final analysis the extent of health care provided decides who lives or survives, to what extent people live in pain and suffering, and who dies.2
How can social health insurance institutions be organized in a more future-oriented way?
The question about organizing social health insurance systems in a more future-oriented way is central to the problem of a balanced relationship between the public and private sectors, or mixed approaches between the two, such as mutual benefit societies. Profitor non-profit-oriented institutions that are public or private can exist alongside non-profit-oriented public institutions which provide health services. The deciding factor in all cases should be the extent to which such approaches positively influence efficiency and health care provision for the population.
What solutions lead the way out of structural problems for health insurance systems, such as population ageing and associated pressures on costs?
It is becoming increasingly clear in many countries that health insurance systems will have to focus benefits more tightly on the needs of the population. This is particularly true for sectors such as prevention, rehabilitation, primary care and long-term care for an ageing population. Many systems show deficits in these areas, which ultimately lead to increased costs.
The results of the reform debate, which has gone on for many years in some cases, about the questions raised above often contain innovative ideas for reform that could transcend national boundaries. The debate sees great opportunities in
• a future-oriented extension of health insurance with the framework of social protection;
• a progressive development of funding methods;
• an appropriate exertion of influence on expenditure;
• bringing benefits into line with what is actually needed;
• the use of technological advances.
The aim of this publication is to present those important innovations to social health insurance systems in industrialized and developing countries that have been brought in over recent years and, as far as possible, already evaluated. In doing so, the intention is to show the developments that are valid for more than one country which could be relevant in the longer term for taking health insurance systems forward.
The International Social Security Association (ISSAj intends, with this publication, a deeper exchange of experience between differing regions, countries, and health insurance systems, thus providing ideas for politicians and practitioners, scientists, and other experts.
The publication will concentrate on innovations in health insurance policy in the areas mentioned above taken from selected countries in
• Africa, using Morocco and Zimbabwe as examples;
• America, using Uruguay and the United States, amongst others, as examples;
• Asia, particularly India, China, Japan and Vietnam;
• Europe, particularly France and Germany,
for presentation and analysis. In addition this publication will address recent institutional economic findings and selected questions with regard to information technology in health insurance systems from a fundamental point of view.
The publication is divided into six parts dealing with the following topics:
• New approaches in extending coverage in a health insurance system
Aviva Ron and Wouter van Ginneken report on new approaches to extending social protection against illness for those in work in formal and informal economic sectors. Both authors use examples from developing countries.
• Confronting resource scarcity: Innovative strategies
William Newbrander and Rena Eichler refer to the history, organization, and future of successful methods to limit costs through Managed Care in the United States. Aidi Hu presents in detail innovative aspects of health insurance in China combining the pro-rata approach with capital-based coverage.
• Refining benefits to meet current needs
Werner Müller-Fahrnow, Thomas Hansmeier, and Karla Spyra report on trends in benefits, which are characterized, among other things, by improved integration of prevention and rehabilitation programs. Xenia Scheil-Adlung and Naoki Iguchi present innovative solutions for those in need of long-term care from selected countries in Europe and Asia, and analyze the extent to which population trends are being overcome from the point of view of social health care systems.
• New institutional and administrative frameworks
What new institutional and administrative solutions have characterized trends in health care systems over recent years? Aviva Ron addresses basic issues here while Navin Girishankar, April Harding, and Alexander Preker present recent new findings from the institutional economic field and examine the changing role of the state in particular. Practical solutions from Africa, Europe and Latin America, using the example of mutual benefit societies, are presented by Maurice Duranton, Abdellatif Zuaq, and Julio Pilón.
• Transformation through information technology systems
Great importance is also attached to information technology systems in changing the field of health insurance. In particular these can be used to achieve improved efficiency and make use of any rationalization possibilities that remain. Claude Delaveau comments on the fundamental possibilities offered by information technology systems. Gerhard Brenner presents aims, requirements, barriers, and components in his contribution, while Bernd Blobel deals with the problems of data protection in detail.
Many of the innovations presented here have already been integrated into existing reforms and the authors refer to concrete developments in individual countries and regions. In order to give the reader the possibility of forming an opinion on innovative approaches in individual countries in a wider context, a brief overview follows of recent trends and reforms in selected health insurance systems in various regions, and covers innovations in both health care benefits and cash sickness allowances in the systems reviewed.
Recent Trends in Health Care Systems in Africa: The Introduction and Further Development of Statutory Insurance Schemes
Many African countries have set up their health care systems as insurance-based systems and established successful mutual benefit societies,3 particularly in North Africa. The efforts directed at setting up health care systems throughout the rest of Africa can be characterized as the introduction and further development of statutory insurance schemes.
As shown in table 1.2, these efforts refer to the creation of health insurance schemes in Burundi, Kenya, Namibia, the Sudan, and South Africa.
The starting point for the reform efforts in almo...