![]()
1
The laboratory and imaging approaches to thyroid disorders
Jacqueline Jonklaas and David S. Cooper
Introduction
Physiology of the hypothalamic-pituitary-thyroid axis
Laboratory evaluation of thyroid function
Assays of thyroid hormones
Total serum iodothyronine concentrations
Determination of free T4 and T3 concentrations
Causes of increased T4 and/or T3 concentrations
Causes of decreased T4 and/or T3 concentrations
Assays of thyroid-stimulating hormones
Causes of hypothyrotropinemia
Causes of hyperthyrotropinemia
Specialized studies of thyroid function
Thyroglobulin
Thyroid autoantibodies
Tissue responses to thyroid hormone action
Laboratory evaluation for thyroid disease
Screening and case findings
Imaging approach to thyroid disease
Ultrasonography and nuclear medicine studies
Ultrasonography
Technique
Indications
Normal thyroid appearance
Diffuse thyroid disease
Thyroid nodules
Risk stratification systems for thyroid nodules
Lymph nodes
Nuclear medicine studies
Technique
Indications
Normal thyroid appearance
Diffuse thyroid disease
Thyroid nodules
Ectopic thyroid tissue
Thyroid cancer
References
Introduction
The central role of the thyroid gland in controlling metabolism was recognized in the 19th century, but evaluation of the function of the thyroid remains an evolving science. Initial approaches to the assessment of thyroid function centered on measuring end-organ responses as biological markers of thyroid hormone actions. Development of in vitro competitive binding assay methods allowed the direct quantification of hormone levels in serum, and sensitive immunoassays have demonstrated the subtleties of pituitary and hypothalamic control of the thyroid. Abnormalities of hormone binding by serum proteins necessitated sensitive estimation of free hormone levels. With the detection of serum markers of autoimmune and malignant diseases of the thyroid gland, earlier diagnosis and improved monitoring of these conditions have been achieved, often with greater sensitivity than may be clinically relevant. Limitations to the measurement methods utilized exist, however, particularly when underlying assumptions about the comparability of patient and control specimens are invalid. Nonetheless, the clinician can now effectively confirm suspected diagnoses of thyroid dysfunction, cost-effectively screen asymptomatic populations for common diseases, and appropriately monitor the treatment of patients with disorders of the thyroid.
Physiology of the hypothalamic-pituitary-thyroid axis
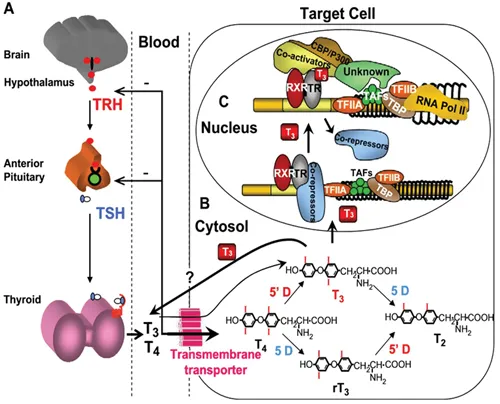
Excellent reviews and books provide detailed explorations of the physiology of the hypothalamic-pituitary-thyroid axis, and the reader is invited to delve into those worthwhile sources (1). For the purposes of this chapter, a brief review of the biosynthesis and transport of thyroid hormones and the regulation of thyroid function by the hypothalamic-pituitary complex will suffice (Figure 1.1).
Figure 1.1 The hypothalamic pituitary thyroid axis. (From Refetoff S, Dumitrescu A. Best Pract Res Clin Endocrinol Metab. 2007;21:277–305. Used with permission.)
The synthesis of thyroxine (T4) and triiodothyronine (T3) begins with the active transport of iodide into the cell via a sodium-iodine symporter located in the basal membrane. Following oxidation by thyroid peroxidase, the iodide moiety is covalently attached to tyrosyl residues of thyroglobulin, and the resulting iodotyrosines are coupled and cleaved from thyroglobulin to form T4 and T3, normally in a 10:1 ratio. Thyroid hormone secretion requires endocytosis and degradation of iodinated thyroglobulin, followed by the release of T4 and T3 into the circulation. This process results in the total daily output of 80 to 100 µg of T4. In contrast, only 20% of the circulating T3 is produced by the thyroid, the remaining 80% is derived from the enzymatic outer-ring or 5¢-monodeiodination of T4 in extrathyroidal tissues such as the liver, kidney, brain, muscle, and skin. Removal of the inner-ring or 5-iodine of T4 forms the inactive metabolite reverse T3 (rT3). Other inactivating pathways for T4 and T3 include glucuronidation, sulfation, deamination, and cleavage. The normal daily fractional turnover rates for T4 and T3 are 10% and 75%, respectively.
In serum, at least 99.95% of T4 and 99.5% of T3 molecules are bound by the transport proteins thyroxine-binding globulin (TBG), transthyretin (thyroxine-binding prealbumin [TBPA]), and albumin. Although TBG is present in lower concentrations than either transthyretin or albumin, its greater affinity for thyroid hormones makes it the predominant serum carrier of T4 and T3. Variations in binding characteristics among normal and abnormal thyroid hormone-binding proteins are responsible for much of the methodologic limitations in assays that attempt to measure concentrations of free T4 and T3. This large pool of protein-bound hormone provides a stable reservoir that maintains the supply of free, unbound hormone available for transport into the cells. Once within target cells, T4 is further deiodinated to T3, which in the nucleus binds to the thyroid hormone receptor, modulating the transcription of thyroid hormone-responsive genes and producing most of the clinical effects recognized as the metabolic effects of thyroid hormones.
The primary regulatory influence on thyroid gland function is the circulating level of thyrotropin (thyroid stimulating hormone, or TSH). Produced by thyrotroph cells of the anterior pituitary, TSH is a two-subunit glycoprotein, the specificity of which is conferred by its β-subunit; the α-subunit is structurally similar to that of follicle-stimulating hormone, luteinizing hormone, and human chorionic gonadotropin. Negative feedback by T4 and T3 influences TSH synthesis and release, as evidenced by a complex inverse relationship between the concentrations of TSH and free iodothyronine (2, 3). It is likely that each individual has a genetically determined set-point for this TSH/free T4 relationship, based on twin studies (4, 5). TSH levels peak just before nocturnal sleep, and the nadir occurs in the late afternoon; this nocturnal surge is lost early in the course of nonthyroidal illness. TSH levels in various populations conform best to a log-Gaussian rather than Gaussian distribution (6). The hypothalamic tripeptide thyrotropin-releasing hormone (TRH) stimulates TSH secretion and modulates thyrotroph response to altered thyroid hormone levels. In conjunction with the suppressive effects of dopamine, corticosteroids, somatostatin, androgens, and endogenous opioids, TRH may be responsible for modulating the setpoint for the negative feedback loop that controls thyroid hormone levels. Hypothalamic production of TRH itself is regulated by circulating thyroid hormones, as well as by multiple central nervous system factors.
Laboratory evaluation of thyroid function
Assays of thyroid hormones
Total serum iodothyronine concentrations
When concentrations and binding affinities of thyroid hormone-binding proteins are normal, there exists at physiologic equilibrium a direct relationship between levels of total hormone and free hormone (7). Thus, measurement of total iodothyronine concentration can provide a reasonable surrogate for estimating the amount of free iodothyronine present. Either serum or plasma can be used to assay hormone concentrations, although serum is generally preferred. The most commonly employed technique for the determination of total T4 (TT4) and T3 (TT3) concentrations is competitive immunoassay, using either polyclonal or monoclonal “capture” antibodies directed against the specific iodothyronine. To ensure measurement of bound as well as free hormones, inhibitors of iodothyronine binding are added—e.g., 8-anilino-1-naphthalene sulfonic or salicylic acids for TBG and barbital for TBPA. These agents successfully dissociate the hormone from binding proteins without interfering with hormone binding to immunoglobulin.
Radioimmunoassay (RIA) d...