This volume addresses the problems the OT profession faces recruiting students into mental health as a practice specialty. The content reflects several efforts at engaging students in the exploration of the variety of available career paths in this area.
Educators, supervisors, clinicians, and students facing career choices will be able to take a unique perspective on specialty selection after reviewing the thoughts, perspectives, theories, and philosophies of some of occupational therapy's foremost leaders in mental health. In addition, readers will get an "up close" opportunity to review one institution's efforts to educate and recruit level II fieldwork students through an all-day program designed to expose them to the widest possible range of practice opportunities.
eBook - ePub
Student Recruitment in Psychosocial Occupational Therapy
Intergenerational Approaches
- 84 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Student Recruitment in Psychosocial Occupational Therapy
Intergenerational Approaches
About this book
Information
A Review, Reflections and Recommendations: Specialty Preference of Mental Health in Occupational Therapy
Anne Hiller Scott, MA, OTR, FAOTA
SUMMARY. It is sobering to consider that the majority of occupational therapy students have fieldwork experiences in mental health and physical disabilities and yet less than 15% choose practice in mental health. How can one account for the limited interest of students in mental health in a field that strongly espouses a holistic approach to patients? This article explores and reviews potential parameters affecting the specialty choice of mental health, to encourage further clarification of problems, identify areas for research and foster creative problem solving. Several theoretical lenses will be suggested to promote clearer focus on conceptual approaches to understanding practice preferences. The occupational therapy literature will be reviewed focusing on personality characteristics, learning style, academic and fieldwork experience and job satisfaction. Additional perspectives including specialization, reality shock, and discontinuity between the academic and clinical phases of professional training are offered from the literature on professional socialization as viable models for understanding this phenomenon. To reverse the trend of declining numbers of practitioners in mental health, recommendations are made for recruitment, academic and clinical education and practice.
A projected increase for occupational therapy personnel of 59.8% is forecast through 1990 (“OT Among,” 1986) and the demand for therapists currently exceeds the output of educational programs (“OT Shortages,” 1989). However, decreasing numbers of therapists are pursuing positions in mental health creating a manpower crisis in this specialty area. The profession is mobilizing resources to develop broadly based strategies to reverse this trend and revitalize mental health practice (Baum, 1983; Bonder, 1987; Kolodner, Wiener & Frum, 1989). The intent of this article is to review literature from occupational therapy and other fields germane to specialty selection, reflect on critical issues for mental health practice and recommend viable approaches to stimulate renewal.
INTRODUCTION: SPECIALIZATION OR WHAT’S IN A NAME
What is specialization and how do therapists classify their interventions? At any point in time how many therapists are practicing in a given specialty area? Although a critical point to the thesis of declining numbers in mental health is accurate documentation of shifts in personnel distribution, obtaining a representative census is not so straightforward. Before describing the distribution of therapists by specialty area, some caution is required due to overlap in definitions of specialty and differing approaches to classifying specialty areas.
Historical and longstanding distinctions acknowledged the areas of physical disabilities, mental health, gerontology and pediatrics. With the benefit of enabling legislation (Public Law 94-142), pediatrics has expanded considerably in the last decade to encompass 25% of practitioners. The American Occupational Therapy Association (AOTA) officially adopted special interest sections in 1978 and designated the areas of physical disabilities, mental health, developmental disabilities, gerontology and sensory integration. Recently the areas of administration and work programs have been added and new groups are forming in education, private practice and holistic practice. These classifications are not mutually exclusive and also represent different dimensions of categorization, e.g., age of patient (gerontology), type of disorder (mental or physical), age of onset of disorder (developmental disability), and type of intervention (sensory integration, work programs). For example, therapists often identify pediatrics as a specialty area and may be referring to working with children who have physical handicaps or developmental disabilities with sensory integration approaches. Some researchers have examined specialty preference as including mental health, physical disabilities, and pediatrics (Christie, Joyce & Moeller, 1985a), others used these categories and gerontology (Ezersky, Havazelet, Levenson, Scott & Zettler, 1985; Leonardelli & Caruso, 1986) or have used the AOTA designations of mental health, physical disabilities, developmental disabilities, gerontology and sensory integration (Swinehart & Wittman, 1988).
Specialty definition also raises concern regarding the holistic orientation of therapists. Breines (1986, 1987) suggested that the profession abandon specialty distinctions in favor of adopting an integrated identity and holistic approach to patients regardless of disability area. It is important to recognize the limitations of our current classification of specialty areas and advise future researchers to include relevant dimensions in analyzing specialty, such as type of disorder, age of patient, and even type of institutional setting to accurately capture salient characteristics of practice.
Little is known about how stable or fluid therapists are in their committment to practice in various specialty areas. There is a need to investigate tenure in specialty practice, occurrence and direction of shifts and factors which contribute to these shifts. There is some indication that as therapists move from their first to their second position, they leave practice in mental health and gerontology for positions in pediatrics and physical disabilities (Ezersky, Havazelet, Levenson, Scott & Zettler, 1985). Canadian researchers have begun to develop data regarding career patterns and influences contributing to changes of position (Madill, Brintnell, Stewin, Fitzsimmons & Macnab, 1985).
LITERATURE REVIEW
The following review includes studies relevant to specialty preference in occupational therapy and related health fields. Topics include specialty preference, personality characteristics, learning style, academic and clinical education, job satisfaction, and professional socialization.
Specialty Preference
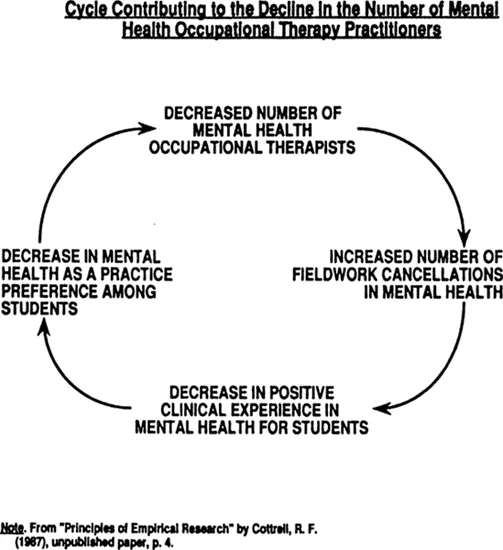
The progressive decline of therapists practicing in mental health has persisted for more than a decade and is affecting the viability of this specialty area. Although the absolute numbers selecting mental health has not declined, the overall percentage of therapists specializing in mental health has decreased from 18% in 1973 to 8.5% in 1986 (“1986 Member,” 1987). Cottrel (1987) has illustrated the corrosive impact of the declining number of practitioners (see Figure 1) reducing manpower resources, curtailing educational experiences for student training and reducing the availability of services for patients. Due to staffing shortages, mental health fieldwork experiences are among the most frequently cancelled compromising the potential for exposure to dynamic clinical sites (AOTA, 1987).
Personality Characteristics
How might personality characteristics contribute to favorable disposition towards various specialty areas? Brollier (1970) compared occupational therapists working in mental health and physical disabilities using the Edwards Personal Preference Scale. Occupational therapists working in physical disabilities were compared to physical therapists; and occupational therapists in mental health to social workers. The scores for each group of occupational therapists were similar to the professions to which they were matched. In addition, there were significant differences between occupational therapists in the two specialty areas. The mental health sample scored higher on dominance and autonomy; the physical disability group were lower on autonomy and deference and higher on order. The two groups were similar on variables of intraception, nurturance and achievement. It was concluded that differences in personality needs correlated with the different focuses in practice vis a vis content of practice, patient/therapist relationship and team interaction. Hendrickson (1962) studied a sample of psychiatric occupational therapists using the 16PF (16 Personality Factors) and also found high values on dominance and a related factor of being tough and self-reliant.
Figure 1
Learning Style
Stafford (1986) examined the influence of learning style on Level II Fieldwork Performance for physical disability and mental health experiences. The instruments used were the LSI (Learning Style Inventory) (Kolb, 1976, 1984) and the SOLAT (Your Style of Learning) (Torrance & Reynolds, 1980). A preference for active experimentation contributed positively to performance in each specialty area. In physical disabilities, scores were enhanced by a logical, sequential cognitive style, but these same qualities negatively affected some of the scores on the fieldwork performance instrument in mental health settings.
In nursing and medicine there has been some correspondence noted between learning style and specialty preference (Laschinger & Boss, 1984; Plovnick, 1975). Plovnick (1975) noted that medical students initial career preferences related to learning style and environmental factors, specifically courses and role models. Students who were more concrete learners as indicated by the LSI were more affected than others by the clinical work experience and attractive role models. Students selecting psychiatry demonstrated the divergent learning style incorporating use of concrete experience and reflective observation. Kolb (1981), the author of the LSI proposed that individuals chose fields that were compatible with their learning style and were further influenced and shaped by the learning norms of the profession. Occupational therapists fall within the accommodator learning style (Bennett, 1979) favoring concrete experience and active experimentation versus the use of reflective observation and abstract conceptualization.
Research suggests that learning style is a relevant variable impacting on specialty preference, academic and clinical education. Further study is warranted examining the relationship of learning styles of occupational therapy students and clinicians to specialty preference. If the concrete learning style does prevail, it follows that specialty choice may be more likely to be influenced by personal factors (role models and clinical experience) than by coursework, which would be the case for abstract learners.
Learning style would have strong relevance for how basic content is taught as well as how clinical fieldwork is integrated. Two studies noted dislike of academic coursework in mental health as a negative factor on specialty choice (Christie, Joyce & Moeller, 1985a; Ezersky, Havazelet, Levenson, Scott & Zettler, 1985). Feedback indicated that coursework was “… too nebulous, too general, too subjective, lacks empirical method, has no structure, is not concrete enough” (Christie, Joyce & Moeller, 1985a, p. 673). Burra and colleagues (1982) found that the attitudes of occupational therapy students became more negative following a psychiatry course. This finding was interpreted to be reflective of the absence of concomitant clinical exposure with the opportunity to see viable application of the field, rather than just exposure to theoretical material.
Page (1987) surveyed occupational therapy students rejecting mental health and identified rive relevant areas: social stigma associated with the mentally ill, mental health course content, coupled with students cognitive level, dissatisfaction with practice setting (state hospital), and lack of previous experience or exposure. Page elaborated on the dualistic i.e., right or wrong quality of students’ thinking style using Perry’s (1969) developmental stages of ethical and cognitive development. “Students needing instructions, hierarchy and consistently right answers will have difficulty making meaning of multiple factors influencing disordered motivation, emotional response, or cognitive orientation” (Page, 1987, p. 2) of the mentally ill clinical population.
Schwartz (1984) has incorporated an approach to analyzing students’ needs in clinical supervision utilizing Loevinger’s (1977) developmental model of ego stages. The cognitive style at level 3 is characterized by conceptual simplicity and stereotypes, followed by multiplicity and then conceptual complexity. In this author’s experience, students on Level I Fieldwork strongly identify with these descriptions as representative of their cognitive and affective reactions to the clinical experience. Schwartz offers guidelines as well for matching clinical instruction and supervision to the student’s developmental level.
Findings regarding dislike of mental health coursework offer rich opportunity for speculation and further research. Potential studies could examine the relationship of cognitive style to course dislike, the presence, absence or timing of concomitant fieldwork on the integration of mental health content, factors related to the presentation and teaching methodologies employed, the influence of role models, previous exposure to psychiatric populations and attitudes toward the mentally ill.
Academic and Clinical Education
Swinehart & Wittman (1988) investigated specialty preference using AOTA specialty designations. Results indicated relatively minor shifts in specialty preference over the course of academic and clinical education. These findings suggest that specialty preference may be established and relatively firm prior to program admission. Although other investigators (Christie, Joyce & Moeller, 1985a; Ezersky, Havazelet, Scott & Zettler, 1989) have not had similar findings further research is warranted which tracks students’ preferences on a longitudinal basis. One implication of this study is the need to actively recruit occupational therapy applicants attracted to mental health practice from the onset of their educational training.
Christie (1985a) and colleagues examined professional, academic and fieldwork influences on specialty. More than half (57%) of the sample indicated that their preference was not formed when they started the curriculum; 55% noted that their specialty interest developed or changed during fieldwork. The majority of respondents ranked the Level II Fieldwork experience as the primary influence on specialty choice. Smaller percentages, 20% and 16% respectively indicated preprofessional exposure and academic component as the highest ranking factors in their choice. The critical qualities of the fieldwork experience included the supervisor role model, communication/relationships, the attitudinal environment and variety in learning experiences and caseload. Effective supervision demonstrating the appropriate attitudinal and interpersonal variables was the most critical parameter of a positive clinical learning experience.
Christie and colleagues (1985b) elaborated on ef...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- About the Editor
- Preface: Education and Enticement: A Recruitment Strategy
- A Review, Reflections and Recommendations: Specialty Preference of Mental Health in Occupational Therapy
- Enriching the Fieldwork II Experience: A Recruitment Strategy for Psychosocial Occupational Therapy
- A Mid-Career Perspective of Mental Health Practice
- The Promise of Occupational Therapy: Professional Challenges, Personal Rewards
- Reflections on Choice
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Student Recruitment in Psychosocial Occupational Therapy by Susan Haiman,Diane Gibson in PDF and/or ePUB format, as well as other popular books in Medicina & Formación médica. We have over 1.5 million books available in our catalogue for you to explore.