eBook - ePub
Practical Management of Affective Disorders in Older People
A Multi-Professional Approach
- 272 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Practical Management of Affective Disorders in Older People
A Multi-Professional Approach
About this book
Building on the success of "Practical Psychiatry of Old Age" now in its Fourth Edition, this book looks in more detail at affective disorders from a variety of perspectives. It includes expert contributions on areas such as aetiology, diagnosis and psychological and pharmacological treatment. It also focuses on a contextual approach to the management of affective disorders in areas like primary care and geriatric medicine, as well as the specific contributions of disciplines such as nursing, social work and occupational therapy. User and carer viewpoints are also included, along with the often neglected spiritual aspects of managing these conditions. This balanced, inclusive and practical approach makes it ideal for all members of the multi-disciplinary team involved in the management of affective disorders in older people.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
GeriatricsCHAPTER 1
Affective disorders in the new millennium
John P Wattis
Introduction
While concepts of depressed mood or melancholia have been with us for many centuries, it is only in the last 50 years or so that our understanding of the biochemistry and physiology of depression (and mania) have advanced significantly. ‘Evidence-based’ psychological and psychopharmacological treatments are also relatively recent, though the roots of psychodynamic therapy go back a little further. The whole evidence-based approach to healthcare1 has resulted in a more standardised approach to treatment, exemplified in the National Institute for Clinical Excellence (NICE) guidance on the management of depression.2 The social, political and economic contexts of psychiatric practice are changing rapidly. In the Western world the nuclear family has largely replaced the extended family and capitalism is now the dominant economic system worldwide. People in the richer countries have access to a wide range of treatments for mental disorder though these may be constrained in different ways depending on how healthcare is funded. Improvements in communication and the phenomenon of ‘globalisation’ have brought different cultures, religions and world-views into contact, sometimes resulting in positive collaborations and synthesis and sometimes in conflict.
Two trends are particularly relevant to the subject of affective disorders in old age at the beginning of the new millennium. The first is the vast shift in the age structure of the population, now affecting virtually all continents and cultures. Many developed countries now have 15% or more of the population in the over- 65-years age group and numbers are increasing across the world. In the UK, the proportion of the population aged 65 and over has increased from around 5% in 1900 to around 16% currently. Over the period 1971–2005, the percentage of people aged 65 and over increased from 13% to 16%. Within this age group even greater increases were seen for those aged 85 and over. The proportion of those aged 65 and over who were aged 85 and over increased from 7% in mid-1971 to 12% in mid-2005. The Office of National Statistics predicts that population ageing will continue during the first half of this century, since the proportion of the population aged 65 and over will increase as the large numbers of people born after the Second World War and during the 1960s baby boom become older. The proportion of population at working ages is set to fall as the baby boomers move into retirement and are replaced by the smaller numbers of people born in each year since the 1960s.3 Reduced infant mortality and better healthcare generally now mean that other countries are undergoing a similar demographic shift.
The second major trend is the increasing synthesis of psychological, social, physical, spiritual and pharmacological viewpoints in the understanding and management of affective disorders. Biomedical sciences are no longer seen as necessarily in opposition to the ‘softer’ psychosocial sciences and the false opposition between science and religion is weakening. This is reflected in the contents and multidisciplinary authorship of this volume.
Depression is an important cause of morbidity and mortality in old age. Mania is much less common but can have a devastating impact when it does occur. In this introductory chapter we will first consider depression in some detail. Then we will consider mania and hypomania more briefly. In this overview, there will inevitably be some overlap with the contents of the chapters that follow and we will point to these as appropriate.
Depression
In this section we will consider the following.

- associations with physical illness and disability/handicap
- exercise
- gender differences
- detection and measurement of outcome.
Clinical features
Severe depression changes life completely. It affects behaviour, relationships, emotions, motivation, thinking, sleep and other somatic functions. The person who could mix well socially suddenly becomes isolated and reclusive. Everything is too much trouble. Personal appearance is neglected and the capacity for enjoyment is reduced. Appetite is often diminished, food is not enjoyed and weight is lost (though sometimes ‘comfort eating’ leads to weight gain). Often sleep is disrupted and waking early in the morning may be compounded by diurnal variation of mood with mood generally (but not always) worse first thing. Severe depression reduces motivation and slows mind and body. It distorts thinking and even memories, resulting in preoccupation with negative themes such as poor physical health, guilt, self-reproach and unworthiness. Agitation sometimes complicates depression and may paralyse the patient’s capacity to make decisions or manifest itself in constant seeking for comfort and reassurance. Weepiness is more common in women than men but is often reported indirectly by friends, relatives and carers since the patient may feel she has to conceal her true feelings from strangers. Suicide risk is high, especially in men. Depression in older men differs in a number of respects from depression in older women (this is discussed in more detail in a later section).
Classification and definitions
The major international system for classifying diseases, The International Classification of Diseases, 10th edition (ICD-10),4 groups all mood disorders together under seven main categories as follows:
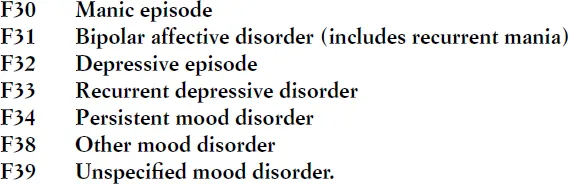
Each category is subdivided according to severity (mild, moderate or severe) and the presence or absence of psychotic symptoms. There are also coding provisions to record the presence or absence of somatic symptoms (anhedonia, mood worse in the morning and early morning waking). This generates around 30 different categories for depression, though in practice some are more common than others.
Unfortunately, the need for consistency in diagnosis can generate very complicated rules. For example, a diagnosis of mild depressive episode rests on the following:
- The syndrome must be present for at least two weeks, there must be no history of mania/hypomania and the depression must not be attributable to organic disease or psychoactive substances (the difficulty of this will become evident when we examine associations with physical illness in more detail).
- At least two of the following three symptoms must be present:
- Depressed mood to a degree that is definitely abnormal for the individual, present for most of the day and for almost every day, and largely uninfluenced by circumstances
- Loss of interest or pleasure in activities that are normally pleasurable
- Decreased energy or increased fatiguability.
- Additional symptoms from the following list to give a total of at least four:
- Loss of confidence or self-esteem
- Unreasonable self-reproach or excessive and inappropriate guilt
- Recurrent thoughts of death or suicide; suicidal behaviour
- Complaints or evidence of diminished ability to think or concentrate, such as indecisiveness or vacillation
- Change in psychomotor activity with agitation or retardation (either subjective or objective)
- Sleep disturbance
- Change in appetite/weight.
To be classified as moderate, at least two symptoms from list 2 above and additional symptoms from section 3, to a total of six, must be present. To meet the criteria for severe depression: all three symptoms from section 2 must be present and at least five from section 3 (at least eight symptoms from 2 and 3 in total).
Depressive episodes (F32), whether or not occurring in the context of recurrent depressive disorder (F33) or bipolar disorders (F31), and manic or hypomanic episodes (F30) are our main concern in this volume. However, dysthymia (F34.1) is also important. It describes people whose outlook is persistently depressed but whose depression is not sufficiently severe or acute in onset to be described as a depressive episode. Anxiety symptoms are often prominent. The relationship between dysthymia and depressive disorder is not exclusive. Dysthymia may follow or complicate a depressive episode and it is not always clear that they are different conditions either in terms of causation or treatment.
Epidemiologists and others who research into the relationships between depression and other conditions in old age often resort to less complicated definitions. The main diagnostic classifications (and the rating scales developed from them) have largely been developed in relation to younger adult patients and may not always be ap...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- Foreword
- Preface
- About the editors
- Contributor
- 1 Affective disorders in the new millennium
- 2 Affective disorders in old age: detection and clinical features
- 3 Aetiology of late-life affective disorders
- 4 Pharmacological management of depression in older people
- 5 Pharmacological treatment of bipolar affective disorder in old age
- 6 Electricity, magnetism and mood
- 7 Psychotherapy with older people
- 8 Depression in physically ill older patients
- 9 Relationship between physical illness and affective disorders
- 10 Depression in primary care
- 11 The role of the nurse in the assessment, diagnosis and management of patients with affective disorders
- 12 Occupational therapy and affective disorders
- 13 Social services for older people with depression
- 14 Carer and service user perspectives of affective disorders in older adults
- 15 Cultural aspects of affective disorders in older people
- 16 Religion/spirituality and depression in old age
- 17 An overview of human drug development
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Practical Management of Affective Disorders in Older People by Stephen Curran,John Wattis in PDF and/or ePUB format, as well as other popular books in Medicine & Geriatrics. We have over 1.5 million books available in our catalogue for you to explore.