- 128 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Medical partnerships are highly complex legal and financial entities. This book navigates the reader through the key issues and deals with the less tangible aspects such as partnership dynamics and organisational behaviour. Examples illustrate common difficulties and offer possible choices. It is clear, practical and readable and essential for all GPs entering a partnership. It is also relevant for GPs currently in partnerships, practices considering their partnership deed, Senior House Officers and GP registrars.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Health Care Delivery1
Core values and the practice ideals
Key moral and professional stances
These are the issues that give a practice its character, and are expressions of the core beliefs of the practice. We all have core values although we may not think of them as such, and it is these that make us choose to work very hard, or to be laid back, to fight for justice, or to grab for ourselves, to yearn for novelty and truth, or to stick with the familiar. Values such as this may not be easy to identify, but when the general practitioner partnership is faced with choices, or put under stress (i.e. the everyday life of a practice), they will inform how partners think and behave. If your own core values are out of line with the rest of the practice you will feel uncomfortable, and when the chips are down you are likely to want to make different choices from your partners, resulting in principled disagreement. On the other hand, if all of the partners have identical core values you are likely to become a pretty stereotyped and lopsided practice. Some creative tension is good, to keep debate alive and avoid ‘groupthink’, a state of cosy collusion where no one dares to challenge the party line.
As you work through this book you will be making choices for yourself, which will give you clues to your own core values, but now it may be helpful to spend time reflecting, and write down three key personal core values by which you try to live your professional life (see Box 1.1. and Examples 1–3). You may wish to refer to this later.
Box 1.1: Three of my personal core values
I practise medicine because:
- _______________________________________________________
- _______________________________________________________
- _______________________________________________________
Example 1
Doctor A was approached by a five-doctor partnership to explore the possibility of becoming the sixth partner. They all knew each other very well professionally and Doctor A often did locum work for the partners, with which they were very impressed. They practised medicine in similar ways and all got on well with each other. However, Doctor A had a core value that he should always try to do the best possible job, otherwise he was letting himself down. The other partners felt that having personal boundaries was important, and so set limits on their working. The workaholic Doctor A felt angry that the other partners laziness’ would diminish his work (and therefore self-worth) and the partners saw his perfectionism as a threat to their self-defences. Doctor A did not join the partnership.
Example 2
Three doctors of different ages and medical styles, from different cultural and ethnic backgrounds all shared the same core value about the immense worth of individual patients, and a shared sense of spirituality, albeit expressed in three different religious traditions. They formed a very strong partnership.
Example 3
With three children at private school and a big mortgage on his home and surgery building. Doctor B needed money! He was hardworking and independent and greatly valued his family’s comfortable lifestyle, which to him was a mark of success. He could not afford to risk a partner not working as hard as he did, so although he had a series of assistants, he never looked for a partner.
The stereotypes and self-labelled identity: the practice culture
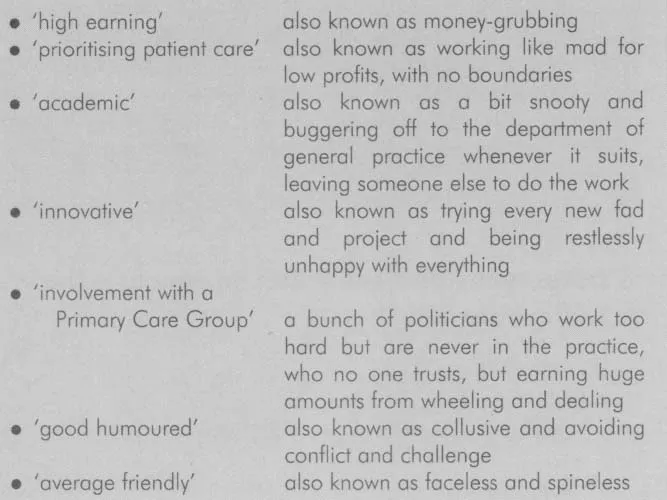
The core values of the practice, together with its collective experience and corporate culture, lead to a practice’s identity. Obviously, there is a whole spectrum of types and styles of practice but some stereotypes can be identified, and often practices will label themselves as ‘friendly’ or ‘academic’, for example. You will see these terms in advertisments, and like those in estate agents, they have double meanings for the cynical (see Box 1.2). They may sound like what you want, but are they what they seem?
On a more serious note, many practices have carefully thought through moral, political, or religious stances with which they identify themselves. Consider what type of practice might suit your core values. Do you want to be in a cooperative practice where each person, from cleaner to partner, earns the same and shares decision making? Are all partners paid-up members of the Medical Practitioners’ Union taking a solid socialist stand? Does the practice take a particular moral stand, for example, on termination of pregnancy? Would you describe yourself as a ‘Christian practice’, or for that matter a ‘Jewish practice’ or is this something you would be looking for? I have not seen ‘Muslim practice’ or any other religious description attached to a practice yet, although I have known practices informally describing themselves with an ethnic label! Where does legitimate unique identity end and cliquish ‘groupthink’ begin?
Box 1.2: Types of practice
Groupthink is a state that any close-knit group of people can get into where their desire to stick together and not rock the boat, overrides their motivation to think clearly and objectively. The group is seen as invulnerable and never wrong, and outsiders are seen with a degree of suspicion. It will be hard to express a view that goes against the ‘party line’ and so there is an illusion of unanimity. Unfortunately, this leads to a lack of debate and a reluctance to seek outside advice. If a practice ends up like this it can be painful to break out, but the danger of groupthink is that it leads to significant underperformance and therefore poorer patient care.
In many practices, the ethos is not labelled as such, being more an unspoken framework of norms within which members operate, without ever being put into words. The practice may be friendly, caring and hard-working; or disorganised stressed, paranoid and grumpy; respecting the rights of professionals and patients; or self-centred with everyone for themselves. There is also an important balance to be struck between, on the one hand, conflicting values leading to unhelpful confrontation and even open warfare, and on the other, cliquish collusion which, ostrich-like, ignores challenges and rational debate. You can only discover this by talking to people, spending time in the practice and keeping your antennae out.
In the end, all practices are a mixture of good and bad elements, like you, so if you ever find the perfect practice do not join, because you will spoil it!
Training practice status
This is worth considering as an issue in itself, but then as a course organiser I am biased.
Being a training practice carries some professional status and guarantees certain standards, because of the need to be visited for approval every three years. Doctors tend to think of training practices as ‘good’, but patients tend to prefer non-training practices because of better continuity of care.
In practical terms, keeping to the approved standards for training practices can be very expensive in terms of library and consulting room facilities, for example, and is certainly hard work. There is also a lot of educational work to do, with the trainer having a nominal two sessions (two half days) devoted to teaching as well as attending workshops. On the positive side, the practice gains tremendous enrichment from teaching and the whole team is stimulated to develop as fresh ideas are brought in. Education is very infectious. Although always supernumerary to the service needs of a practice a highly skilled professional such as a general practice registrar (GPR) is a very useful person to have around.
Primary Care Group (PCG) involvement
PCGs vary in their structure and workload, from the level 1 advisory role to the health authority through to the very complex level 3 and, in the future, level 4 primary care trust. They also vary greatly in size. One aspect of this is already all too clear. PCGs generate a tremendous amount of work, with internal corporate issues, commissioning, primary care development and clinical governance. This in turn has its impact on practice workload. This will affect all practices, but there will be varying degrees of impact depending on how actively involved with the workings of the PCG the practice wishes to be. If a practice is very involved, with a partner and practice nurse on the PCG board, for example, this will mean a lot of time away from practice business (this appears to be not well reimbursed). On the other hand, the practice will have more influence at PCG level. Conversely, a practice that wants to stay very clinically focused and not play the political game may not have to be distracted too much by the PCG, but could quickly find itself marginalised. Most practices will fall between these extremes and there are plenty of opportunities to be involved in PCG work. However, if partners disagree about how much time should be spent, PCG involvement could become an obvious source of conflict. This is one issue where discussion is necessary in order to avoid any misunderstanding.
2
The partnership dynamic
Team roles
How many partners there are in a practice and how they work together is obviously basic to how the practice runs, but before you make a rapid decision about a practice, consider both your own and your partners’ preferred way of working. Think about how you functioned in the different teams you have experienced.
- Are you good in a team, and why?
- What are your strengths and weaknesses?
- Are you a solitary worker, or a collaborator?
- Are you something of an independent freethinker (others may say a loose cannon)?
- Do you like to have clear rules laid down and work to guidelines and protocols?
- Which role do you tend to play in a team: chair, plant, monitor/ evaluator, team-player (see Box 2.1)?
Obviously, it is desirable to have an eclectic mix within the team – it is chaos if everyone is an independent freethinker, but fossilised if no one ever challenges the status quo!
Some practices do psychological profiling of prospective new partners to see if they are likely to fit into their team often by using questionnaires, but most are not quite that organised (or obsessional).
Work by Beibin* on management teams in industry has shown that the best functioning management teams have a c...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Foreword
- Introduction
- 1 Core values and the practice ideals
- 2 The partnership dynamic
- 3 Owning or leasing the premises
- 4 Financial issues
- 5 How hard do you want to work?
- 6 Working policies
- 7 Final thought
- Appendix: Sources of income and expense
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Partnerships in Practice by Petre Jones in PDF and/or ePUB format, as well as other popular books in Medicine & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.