1 Upper Abdominal
Anu E. Obaro, Venus
Hedayati, Colin R. Deane,
Keshthra Satchithananda and
Paul S. Sidhu
Liver
Liver size
Liver fibrosis assessment
Biliary tree
Gallbladder and gallbladder wall
Spleen
Pancreas
Pancreatic duct (adult)
Adrenal glands (adult)
Diaphragm
Upper Abdominal Vasculature
Portal vein
Hepatic veins
Hepatic artery
Celiac and superior mesenteric arteries
Doppler ultrasound assessment of post-prandial intestinal blood flow
Inferior mesenteric artery
Liver size
Preparation
None.
Position
Supine, right anterior oblique to demonstrate the porta hepatis.
Transducer
2.0–6.0 MHz curvilinear transducer.
Method
Longitudinal views are taken in the midclavicular and midline positions, and measurements obtained. Anteroposterior diameters are also measured at the midpoint of the longitudinal diameters. All measurements are taken on deep inspiration.
Appearance
Uniform pattern of medium-strength echoes.
Measurements
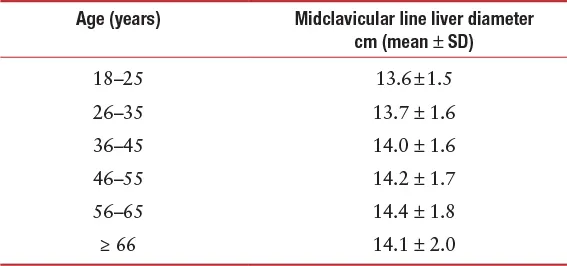
There are significant variations in liver size due to gender, age, body mass index and weight.
Diameter | Female cm (mean ± SD) | Male cm (mean ± SD) |
Midclavicular line (largest craniocaudal diameter) | 14.9 ± 1.6 | 15.1 ± 1.5 |
In the transverse plane, the normal caudate lobe should be less than 2/3 of the size of the right lobe.
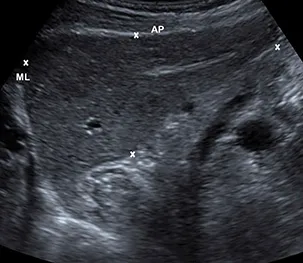
A midline longitudinal view through the left lobe of the liver, demonstrating the anteroposterior diameter (AP) and the midline longitudinal length (ML).
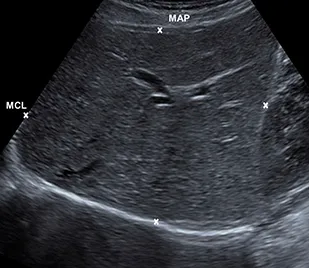
A midclavicular longitudinal view through the right lobe of the liver, with a midclavicular anteroposterior diameter (MAP) and a midclavicular longitudinal length (MCL).
Further Reading
Kratzer W., Fritz V., Mason R.A., Haenle M.M., Kaechele V. Factors affecting liver size: A sonographic survey of 2080 subjects. J Ultrasound Med.2003; 22:1155–1161.
Patzak M, Porzner M, Oeztuerk S, Mason RA, Wilhelm M, Graeter
T, Kratzer W., Haenle M.M., Akinli A.S.. Assessment of liver size by ultrasonography. J Clin Ultrasound.2014; 42:399–404.
Liver fibrosis assessment
Preparation
Patient should fast for 6–8 hours prior to the examination.
Position
Supine, right anterior oblique.
Transducer
2.0–6.0 MHz curvilinear transducer.
Method
Measurements are obtained from an intercostal view, to interrogate an area of the liver at least 2 cm deep to the liver capsule, away from major vessels. The right arm is raised above the head. The sample box is placed over the area selected, ideally in a perpendicular position, and a total of 10 measurements are obtained in brief suspended respiration, from the same area of liver. Segments 5 and 6 are normally interrogated; the left lobe of the liver should be avoided. Different ultrasound machines have different methods of obtaining readings and different display methods, and the readings are not transferable between machines. Transient elastography (TE) or “fibroscan” and acoustic radiation force impulse (ARFI) imaging are the most commonly used methods. A fibroscan does not produce an ultrasound image, and provides measurements in kilopascals (kPa).
Appearance
The measurements can be expressed in velocity of shear wave (m/sec). The level of liver fibrosis is calculated and classified according to the METAVIR (F0–F4) or ISHAK (0–6) scoring system to ascertain normality, the degree of liver fibrosis, or the presence of cirrhosis. The most common diseases for which fibrosis will be assessed are Hepatitis C virus (HCV), Hepatitis B virus (HBV), and alcoholic liver disease.
Measurements
Acoustic radiation force impulse (ARFI) imaging
(usi...